

Background: The use of clavicle reduction osteotomies for shoulder reshaping has proven to be an effective procedure. Having performed over 100 patience for shoulder reduction, or over 200 clavicles treated, the vast majority of patients have been very satisfied with their shoulder shape changes. Because it is a structural shoulder change associated with range of motion of the arm there are understandable concerns as to whether the procedure may cause some adverse functional affects. Also because of the very visible appearance of the clavicle there are also patient concerns about the resultant scar as well as the potential visibility of the fixation hardware used.
The potential risk of decreasing the range of motion of the arm what is investigated before the first clavicle reduction osteotomy was ever performed. Based on extensive information in the orthopedic surgery literature in the non-operative treatment of clavicle fracture’s it is well known that it takes at least a 30% shortening of the original clavicle length before range of arm motion is affected. Most clavicle reduction osteotomies due to technical plate application limitations usually only reduce the length of the clavicle about 15 to 20%. As a result patients have reported in the short term no problems with arm range of motion movements. However, long term clinical outcomes are needed to confirm that short term observation.
While scar outcomes and hardware visibility are aesthetic issues the long term outcome of these assessments are still important. While the incision used to perform the procedure it’s fairly small, usually 3.5 to 4 cms, it does undergo a lot of stretch doing the surgery. This could potentially affect it’s long-term appearance. The clavicle is a very visible bone with a thin soft tissue cover particularly in thin patients. As the most important fixation plate is on the superior surface of the bone it is also relevant if the plate becomes an aesthetic liability as full healing and the soft tissue shrink wrap occurs.

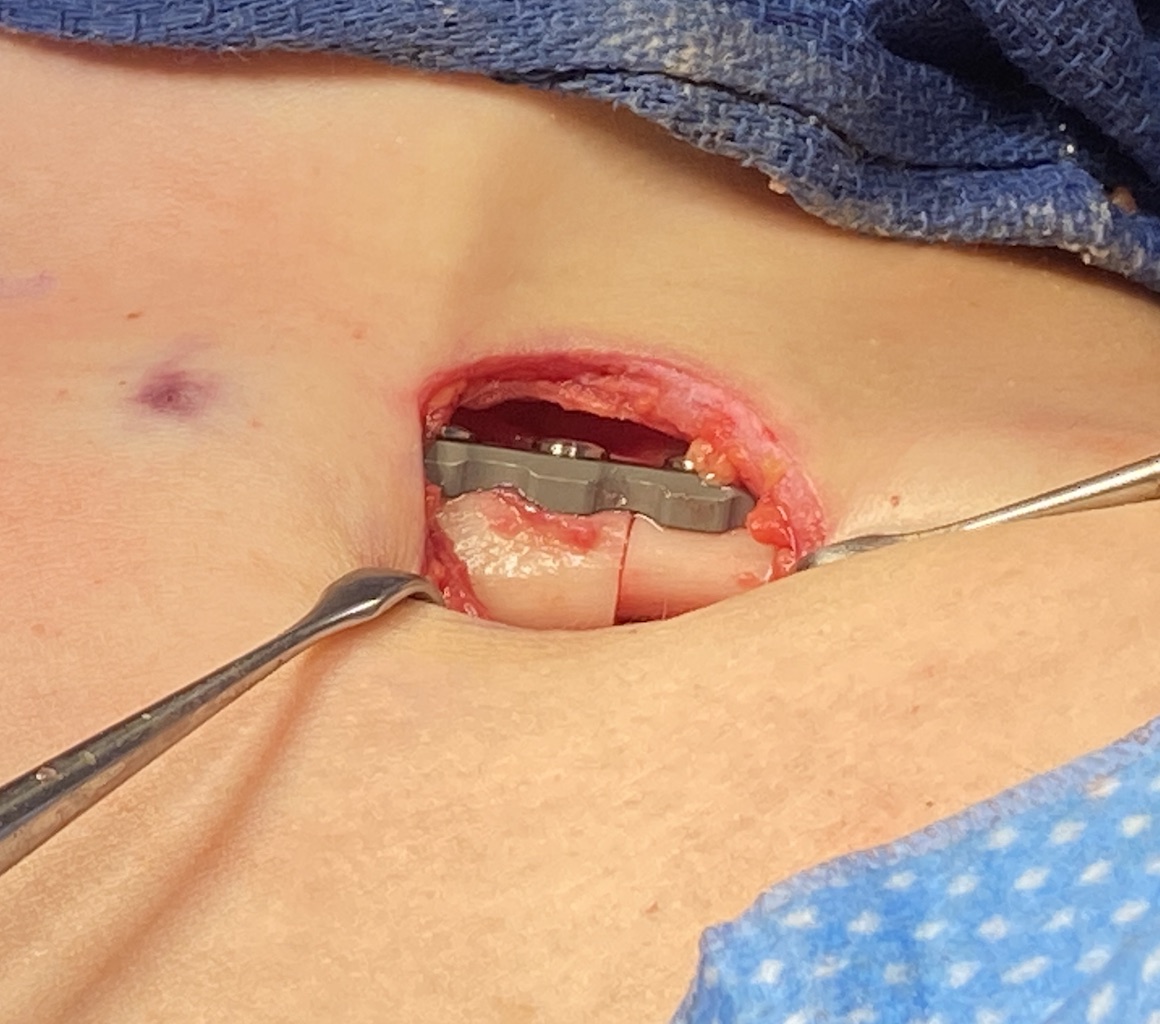
 Case Study: This very thin female desired narrowing of her wide shoulders. She has bilateral clavicle reduction osteotomies with 2.5cms of bone removal on each side. A single superior f3.5mm ixation plate was applied with three bicortical screws own each side. Due to the small size of the clavicle an anterior plate was not used. (to avoid devascularizing the healing of the osteotomy site)
Case Study: This very thin female desired narrowing of her wide shoulders. She has bilateral clavicle reduction osteotomies with 2.5cms of bone removal on each side. A single superior f3.5mm ixation plate was applied with three bicortical screws own each side. Due to the small size of the clavicle an anterior plate was not used. (to avoid devascularizing the healing of the osteotomy site)



 When seen one year later the reductive change in her shoulder shape could be seen. She had no limitations of arm range of motion and there was no rolling in effect of the shoulders. In fact she was a bit disappointed in that regard as she wanted to have some anterior shoulder change which she did not get.
When seen one year later the reductive change in her shoulder shape could be seen. She had no limitations of arm range of motion and there was no rolling in effect of the shoulders. In fact she was a bit disappointed in that regard as she wanted to have some anterior shoulder change which she did not get.

 The incisional scars were barely visible and, while the fixation plate could be felt, it was not visible as such through the skin. It merely made the clavicle look a bit bigger.
The incisional scars were barely visible and, while the fixation plate could be felt, it was not visible as such through the skin. It merely made the clavicle look a bit bigger.
Key Points:
1) Long term results from shoulder reduction surgery shows no functional or range of motion issues.
2) While the shoulders were less wide from side to side there was no anterior rolling in of the shoulders.
3) The clavicle fixation plates are palpable but not be identified as plates visually.
Dr. Barry Eppley
World-Renowned Plastic Surgeon