

Background: The most common chin augmentation requested change s horizontal, increasing its forward projection. This is understandable given that many patients seek improvement of their chin recession. But not all chin recessions are completely horizontal in nature. Vertical chin deficiencies also exist and can occur as a stand alone dimensional deficiency or, more commonly, as part of a horizontal deficiency as well.
The combination horizontal-vertical deficiency is the most frequently underdiagnosed/untreated chin deficiency. This is due to the lack of a recognized off-the-shelf implant to specifically treat it and an appreciation of what moving the chin bone can do. The vertical lengthening chin implant (VLC) is useful in these dimensional chin augmentation needs but is limited to a 45 degree movement and will make the chin wider as well. Custom chin implants can also be used and is not so dimensionally limited. Its limitations arise with the soft tissue chin pad which has limited downward stretch when it is released from the bone.
When significant vertical chin lengthening is needed, as certainly defined as double digit millimeters (10 mms for more) the wedge style bony genioplasty is needed. This means the chin bone is downfractured and a bone graft is placed between the upper and lower bone segments. The amount of vertical lengthening needed becomes the gap between the bone segments. What that gap should be is perioperatively determined by various clinical maneuvers. The most reliable in my experience is the jaw thrust where the patient brings their chin down to the desired position and the measured gap between the upper and lower incisor teeth becomes the amount of vertical chin lengthening needed. It is almost always more than one would think is needed.
Case Study: This male sought surgical improvement of his chin deficiency which he recognized as having a major vertical deficiency. Using the jaw thrust maneuver it was determined that 12mms of vertical length was needed with a few millimeters of forward projection.
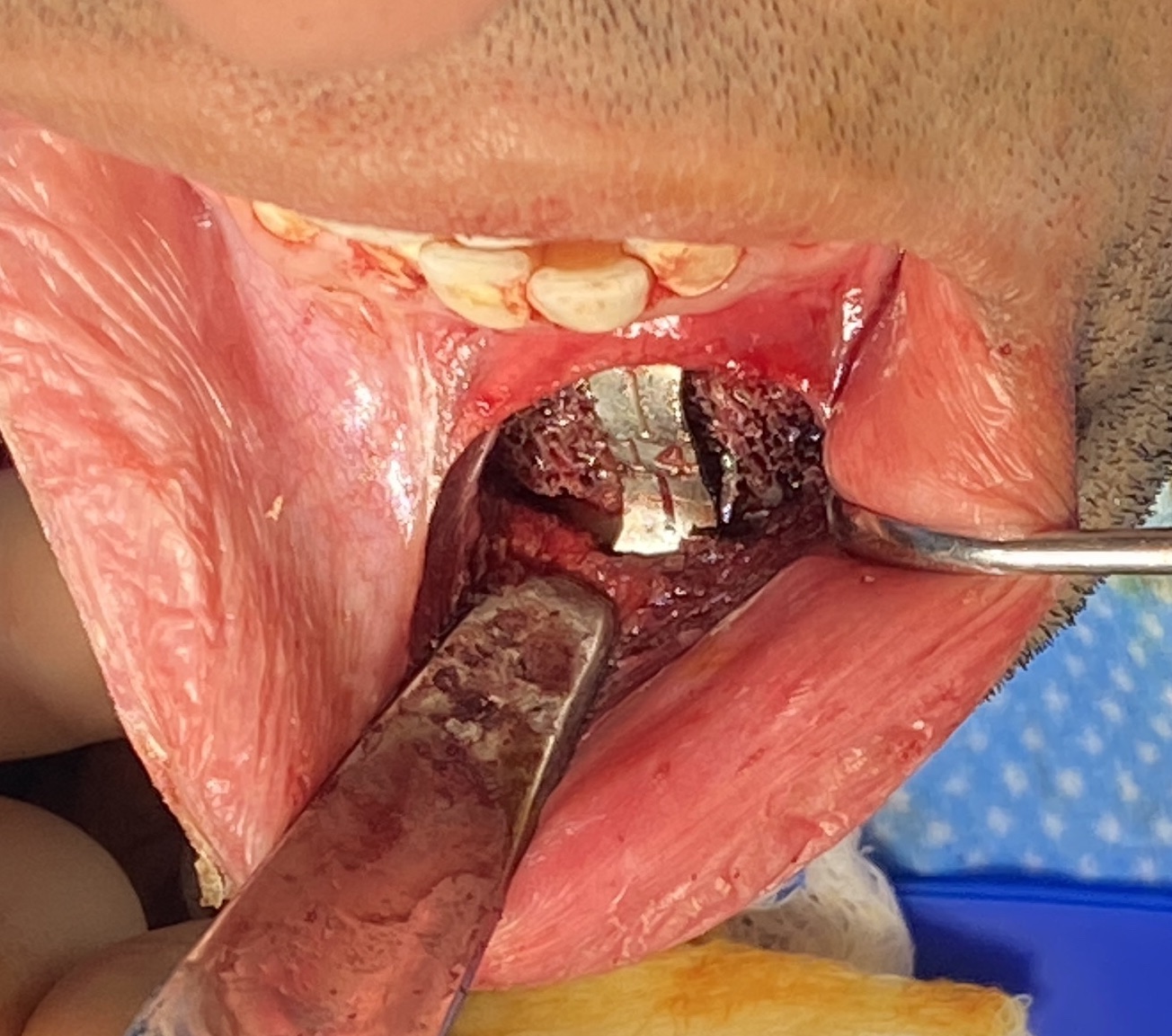
 Under general anesthesia and through a small intraoral incision the bone was down fractured. Using a bent 14mm plate the new chin position was established and secured. A cadaveric corticocancellous bone graft was fashioned to fill in the bone gap as much as possible.
Under general anesthesia and through a small intraoral incision the bone was down fractured. Using a bent 14mm plate the new chin position was established and secured. A cadaveric corticocancellous bone graft was fashioned to fill in the bone gap as much as possible.

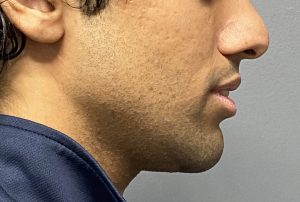

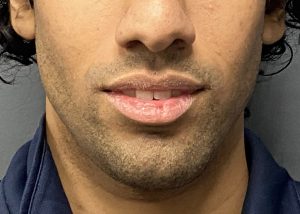 When seen six months later, coincidentally for more vertical chin lengthening, he showed a much improved chin projection.
When seen six months later, coincidentally for more vertical chin lengthening, he showed a much improved chin projection.
Achieving significant lengthening of the chin requires an increase in the height of the bone. Wedging it opens and placing a graft between the twio segments allowed the soft tissue chin pad to follow the bone downward without any risk of chin pad ptosis. Such a bone graft ensures that most of the open gap will fill in with bone long term.
Case Highlights:
1) In the vertically short chin which needs significant lengthening an opening wedge genioplasty with an interpositonal graft is needed.
2) How much the chin need to be vertically lengthened is determined by the patient with the most reliable preoperative determination of interincisal measurement with jaw repositioning.
3) In significant vertical lengthening the amount of lengthening needed is often under estimated as the interincisal meaurement may seem excessive.
Dr. Barry Eppley
World-Renowned Plastic Surgeon