

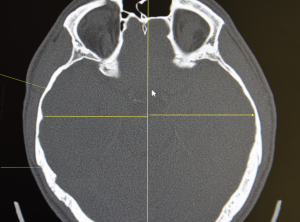
 Background: Of all the skull reduction procedures temporal reduction is the only one that involves removal of soft tissue and not bone. This is because it is the only skull area where the bone is covered by thicker soft tissues than just the five layers of the scalp. The thickness of the side of the head temporal muscle varies but almost always when excessive head width exists the muscle makes a major contribution to it. Whether the muscle or bone makes the greater contribution to the excessive head width, are more equally shared or that the bone is primarily responsible requires a CT scan to accurately make that determination.
Background: Of all the skull reduction procedures temporal reduction is the only one that involves removal of soft tissue and not bone. This is because it is the only skull area where the bone is covered by thicker soft tissues than just the five layers of the scalp. The thickness of the side of the head temporal muscle varies but almost always when excessive head width exists the muscle makes a major contribution to it. Whether the muscle or bone makes the greater contribution to the excessive head width, are more equally shared or that the bone is primarily responsible requires a CT scan to accurately make that determination.
In lieu of a CT scan to determine the effectiveness of muscle removal for head width reduction there is an association between the size of the patient’s head, skin pigment, hair color and ethnicity and the size/thickness of the temporal muscle. There is also the bite test in which the size of the bulge of the muscle on the side of the head is indicative of the potential success of the procedure. Lastly if the width of the head decreases when the mouth is maximally opened this is also a preoperative test of effectiveness.
One potential patient concern with temporal muscle removal is loss of function. It is logical to assume that removal of part of the muscle will result in some loss of jaw opening. But it never has because the bulk of the temporal muscle is in the fossa or concavity of the temporal closer to the eye…which is not where the muscle for head width reduction is removed.
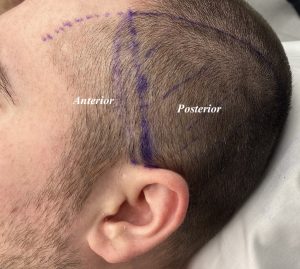
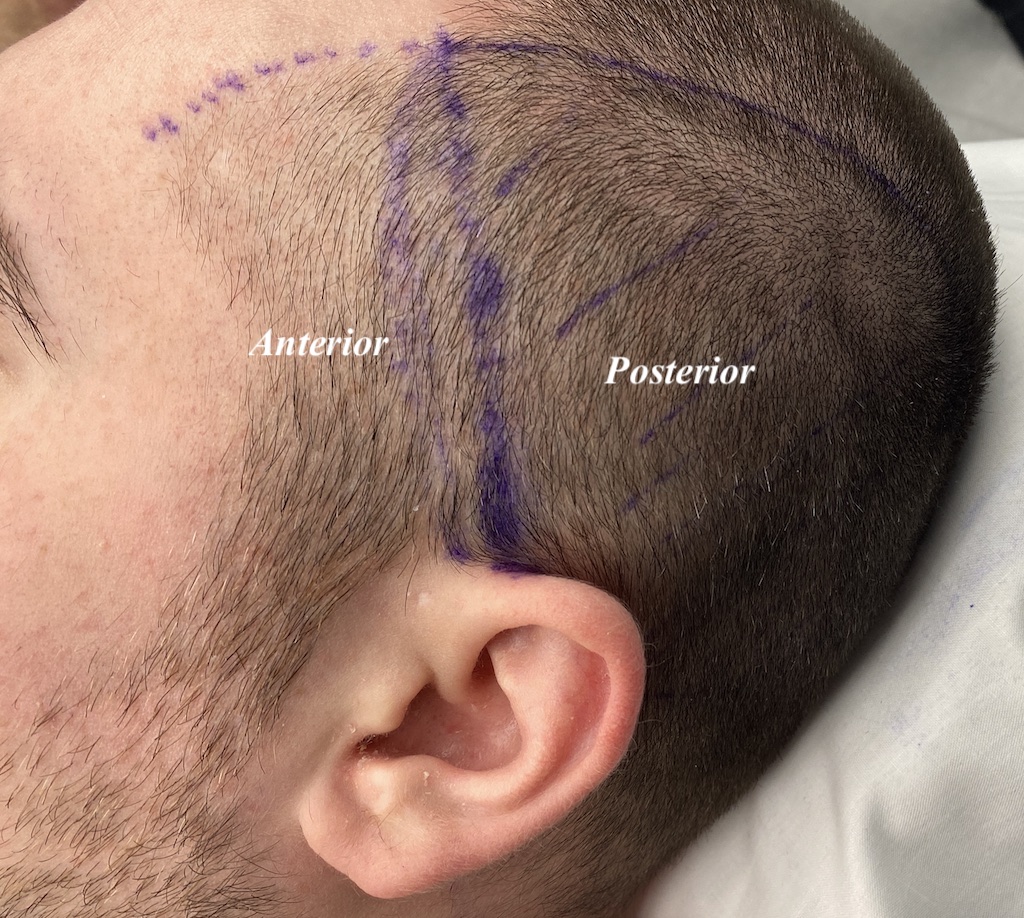
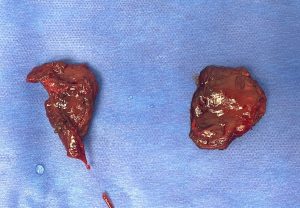 Case Study: This young male was bothered by his wide and convex side of head shape.Under general anesthesia and through postauricular incisions the posterior portion of the temporal muscle was removed leaving the overlying fascia. Large thick muscle segments were removed which shrink down when their attachments are released.
Case Study: This young male was bothered by his wide and convex side of head shape.Under general anesthesia and through postauricular incisions the posterior portion of the temporal muscle was removed leaving the overlying fascia. Large thick muscle segments were removed which shrink down when their attachments are released.

 When seen six months later the improvement in his head shape could be seen with a visible reduction in its width with a straighter profile in the back view.
When seen six months later the improvement in his head shape could be seen with a visible reduction in its width with a straighter profile in the back view.

 In the front view a similar change was seen with a more narrow straighter head profile…although I find it lesser in amount than from the back view.
In the front view a similar change was seen with a more narrow straighter head profile…although I find it lesser in amount than from the back view.
While it it true that the temporal muscle only makes up a portion of the thickness of the side of the head, it represents the easiest target for reduction. With no adverse functional sequelae from subtotal muscle removal and being able to be done in a scarless manner it is the most logical approach to head width reduction. There are more extensive approaches, including temporal bone burring reduction and even temporal scalp tucks, that provide even greater amounts of improvement but at the tradeoff of a visible scar along the side of the head.
Key Points:
1) Temporal reduction is the only effective treatment for an excessively convex or lightbulb-shaped head.
2) Temporal reduction is a scarless soft tissue surgery which removes the posterior portion of the temporal muscle.
3) While counterintuitive removal of a portion of the temporal muscle causes no functional issues. (decreased jaw range of motion)
Dr. Barry Eppley
World-Renowned Plastic Surgeon