


Background: Rib removal is a head of but often not understood procedure. The bottom end of the ribcage are the free floating ribs #11 and #12. Because of this lack of distal attachments that angle down much more significantly than the attached ribs above it. These lack of subcostal/sternal attachments indicates that they do not have any role in respiration which the attached ribs do. Rather they have a structural support role and serve as attachments for various abdominal and back muscles at their cartilaginous ends. They may also provide some role in organ protection for kidneys at their medial halfs.
The angulation of the free floating ribs and their abdominal wall attachments provides an anatomic basis for rib removal surgery for aesthetic waistline narrowing. By removing the outer aspect of these ribs the side of the abdominal wall moves (collapses) inward creating a more inward shape. Since only the outer aspect of the free floating ribs removed no loss of organ protection results.
While the free floating ribs are what is usually perceived as being treated in rib removal surgery the role of the attached rib #10 above them is less well appreciated. While an attached rib it is still useful in torso narrowing. Ideally part of it should be treated along with the free floating ribs for maximal waistlines narrowing effect. But its attached nature make its management more challenging. It is both a thicker rib with a different angulation that is also longer as it wraps around the the torso onto the subcostal ribcage. It also has a closer proximity to the pleura of the base of the lung. As a result it is more difficult to do removal of it from the limited back incision typically used for this surgery. And it does have a risk of pleural violation that ribs #11 and #12 did not have.
Since rib #10 is attached at both ends (the medial end at the vertebral facet is quite rigid while the distal end at the subcostal area is more mobile due to its non-fixed cartilaginous end) it is somewhat like a bridge. An alternative to rib #10 removal is a segmental resection of a small portion of it so the distal end can collapse inward.
Case Study: This female sought waistline shape improvement by rib removal. She had previously bene through BBLK surgery with circumferential waistline liposuction.
 Under general anesthesia in the prone position and through an oblique back incision the distal ends of ribs #11 and #12 were removed,. In addition a segmental resection off rib #10 above it was also performed. A wedge of latissimus dorsi muscle was also removed during closure.
Under general anesthesia in the prone position and through an oblique back incision the distal ends of ribs #11 and #12 were removed,. In addition a segmental resection off rib #10 above it was also performed. A wedge of latissimus dorsi muscle was also removed during closure.

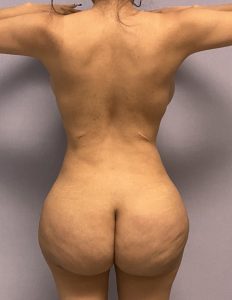 When seen two years later the improvement in the shape of the waistlkine could be seen. The back scars had also healed fairly well given her ingtermediate skin thickness and pigment.
When seen two years later the improvement in the shape of the waistlkine could be seen. The back scars had also healed fairly well given her ingtermediate skin thickness and pigment.
Case Highlights:
1) Traditional rib removal surgery uses an oblique back incision in which ribs 11 and 12 can be removed.
2) Rib #10 can be challenging to remove through an oblique back incision and an option to treat it is a segmental resection as a collapsing maneuver.
3) When seen one year later the improvement in the shape of the waistline can be considered typical.
Dr. Barry Eppley
World-Renowned Plastic Surgeon