

Background: Loose tissues around the waistline and torso are most conventionally treated by a tummy tuck. While this is a good operation for many patients it will not be effective when the primary goal is waistline narrowing because the loose tissue removal is in the wrong direction. A tummy tuck is a horizontal removal which pulls the abdominal wall downward and not inward. A vertical excision is needed, which can be performed on the anterior abdominal wall, but that is rarely a good scar location unless that is where most of the loose tissue resides.
Non-tummy tuck excisional torso body contouring options are very limited. The most commonly known one would be the bra line lift which is a horizontal excision of tissue across the mid-back along the bra line in females. While effective in the right patient this creates a transverse torso tightening effect…somewhat similar to a tummy tuck albeit higher in the back.
Vertical torso tightening operations through excision have rarely been described. Vertical excisions done along the sides of the torso have been done, and while effective, it creates two prominent scar lines. An alternative is to change the excision to a vertical line down the center of the spine creating a corset-like effect when the two sides are brought together. This does result in a long scar but at least it is one scar and is placed in a potentially less visible location on the back.
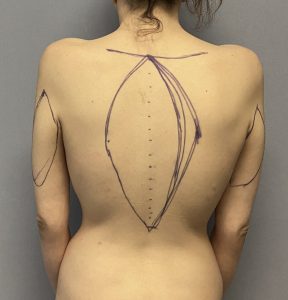 Case Study: This young female has prior weight loss and desired waistline/torso narrowing. By the pinch test she had a good skin mobility in the vertical direction over the spine on her back. She already had a fairly narrow waistline but her torso width above it was much wider. Thus the elliptical excision pattern for the vertical backlift was wider in the upper half than the lower half. The pinch test indicated that the excision pattern could extend to a horizontal line across the top of the scapula. The inferior end went down to stop above the sacral dimple.
Case Study: This young female has prior weight loss and desired waistline/torso narrowing. By the pinch test she had a good skin mobility in the vertical direction over the spine on her back. She already had a fairly narrow waistline but her torso width above it was much wider. Thus the elliptical excision pattern for the vertical backlift was wider in the upper half than the lower half. The pinch test indicated that the excision pattern could extend to a horizontal line across the top of the scapula. The inferior end went down to stop above the sacral dimple.
 Under general anesthesia and in the prone position the vertical excision of skin and fat was completed.
Under general anesthesia and in the prone position the vertical excision of skin and fat was completed.

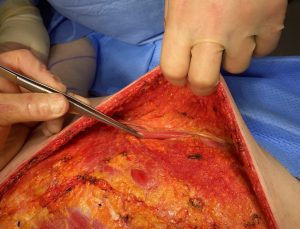 Through the wide open exposure the back flaps were raised to the sides until the lateral border of the LD muscle was identified. A 2 to 3cm strip of the LD muscle was taken and the new lateral muscle border than plicated onto itself by sutures for further torso narrowing.
Through the wide open exposure the back flaps were raised to the sides until the lateral border of the LD muscle was identified. A 2 to 3cm strip of the LD muscle was taken and the new lateral muscle border than plicated onto itself by sutures for further torso narrowing.

 The vertical backlift was then closed over drains in multiple layers with resorbable subcuticular sutures for the skin.
The vertical backlift was then closed over drains in multiple layers with resorbable subcuticular sutures for the skin.
She went on to heal with some early need for seroma aspirations after drain removal and also underwent a scar revision on the lower end of the scar.

 In the long term her torso reduction was visible and the scar was acceptable.…which hopefully the patient viewed as a worthwhile tradeoff.
In the long term her torso reduction was visible and the scar was acceptable.…which hopefully the patient viewed as a worthwhile tradeoff.

 In the front view the toro narrowing effect was very much like a corset pulling in the sides. An effect that was the combined result of the corset pull of the vertical backlift closure and the LD muscle modifications.
In the front view the toro narrowing effect was very much like a corset pulling in the sides. An effect that was the combined result of the corset pull of the vertical backlift closure and the LD muscle modifications.
The obvious drawback to a vertical backlift is the long space down the center of the back. That scar is not necessarily in a well hidden location but in the properly motivated patient it could be a good tradeoff for the torso effect that can be achieved.
Key Points
1) Loose skin around the torso limits how much body reduction contouring is possible from weight loss.
2) When significant loose torso skin exists the vertical backlift acts like a corset and also allows access for rib removal surgery.
3) The vertical backlift scar generally heals well but some patients may require a secondary scar revision for an optimal scar outcome.
Dr. Barry Eppley
World-Renowned Plastic Surgeon