

Background: Clavicle reduction osteotomies have proven to be a safe and effective technique for aesthetic shoulder narrowing. A section of the clavicle bone is removed on the inner half of the clavicle, due to an aesthetically favorable incision location in the supraclavicular fossa, and the distal clavicle segment is brought inward to reunite with the residual medial clavicle bone. The two bone ends held together with titanium fixation hardware and full bone healing is expected similar to that of a clavicle fracture repair. To date, almost all patients have gone to uncomplicated healing Long term as evidence by lack of any reports by the patients of postoperative problems. While an immediate postoperative x-ray is obtained to view and document the bone fixation site long-term postoperative x-rays are not routinely take them to evaluate bone healing as the metal hardware blocks a good radiographic view of the osteotomy site.
While patients can have the fixation hardware removed one year after the surgery very few elect to do so. The reasons for hardware removal would be visible show, irritation from rubbing across the clavicle site or just the desire to not have implanted foreign bodies. In the few patients in whom I have removed their metal hardware I have not observed any non-unions or obvious issues with full bony healing across the osteotomy site. I have yet to take a postoperative x-ray after hardware removal given what I have seen in surgery as well as the few patients who ever had that secondary procedure done. It would be interesting to see how the union of the two bonanza looked radiographically after the hardware is removed.



 Case Study: This female had clavicle reduction osteotomies for shoulder narrowing with removal of 2.5cms. of bone per side. She had an uncomplicated recovery with a return to a full range of motion with a very active lifestyle. (e.g., rock climbing, tennis) She was pleased with the aesthetic outcome. She desired hardware removal two years after the surgery.
Case Study: This female had clavicle reduction osteotomies for shoulder narrowing with removal of 2.5cms. of bone per side. She had an uncomplicated recovery with a return to a full range of motion with a very active lifestyle. (e.g., rock climbing, tennis) She was pleased with the aesthetic outcome. She desired hardware removal two years after the surgery.

 Her supraclavicular scars healed well and were barely perceptible.
Her supraclavicular scars healed well and were barely perceptible.

 Under general anesthesia and through her existing scars the clavicle hardware was exposed and removed. The osteotomy sites showed complete healing across the two bone ends brought together.
Under general anesthesia and through her existing scars the clavicle hardware was exposed and removed. The osteotomy sites showed complete healing across the two bone ends brought together.
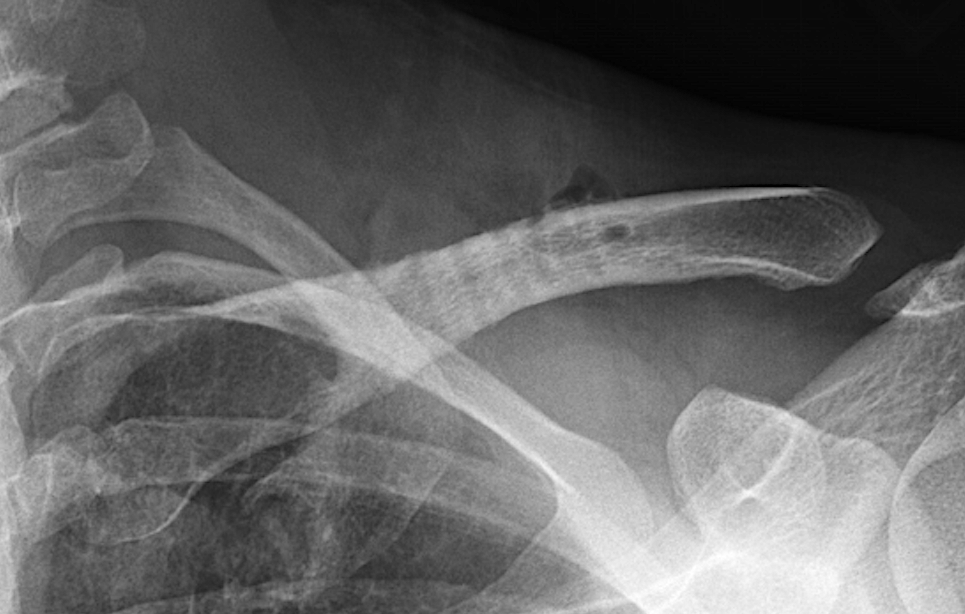
 A postoperative x-ray showed well healed osteotomy sites and residual visible holes in the bone from the 3.5mm screw removals. (which will eventually heal in with bone) The clavicle appears shorter in length with an increased acromio-clavicular joint space.
A postoperative x-ray showed well healed osteotomy sites and residual visible holes in the bone from the 3.5mm screw removals. (which will eventually heal in with bone) The clavicle appears shorter in length with an increased acromio-clavicular joint space.
I advise all patients that they can if they desire to have their clavicle hardware removed one year after surgery. At this point I would expect full bony healing. However, because of potential stress shielding from the hardware, the healed osteotomy site may not actually be a strong as it was before the surgery. It likely takes some time with the return of unsupported load bearing to have the bone return to completely normal strength. There is also the six large residual screw holes, which are not near the osteotomy site, but they will also take some time to heal. Thus I would advise patients for the first month or two after surgery to be cautious about very strenuous physical activities.
Key Points
1) The long term outcome of clavicle reduction scars is very favorable with few patients ever requesting a scar revision.
2) In the few cases seen long term with visual and radiographic analysis the clavicle reduction osteotomy sites have shown full bony healing.
3) Fixation hardware can be removed one year after clavicle reduction surgery with short term visibility of the screw holed which would be expected to fully heal.
Dr. Barry Eppley
World-Renowned Plastic Surgeon