

Background: The shape of the male chest is influenced by a variety of anatomic structures of which the largest is the pectoral muscle. Lying between these soft tissue masses is the bony sternum whose lateral edges are made up of the rib articulations and the attachment origins of the pectoral muscles. As a midline chest structure the bony sternum is generally seen as a smooth, flat and inwardly shaped chest feature.
The sternum or breastbone, which has a necktie type shape, is one of the longest and flattest bones in the body. It is composed of three regions which are the upper manubrium, the longer central body and the inferior xiphoid process. While aesthetically prominent but making up a relatively small area of the entire chest, it plays a vital functional purpose due to the attachment of the ribs to it which both support respiration and protect the heart.
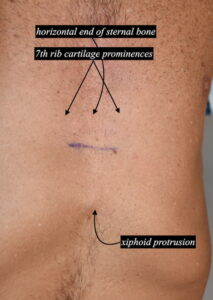
The attachment of the ribs to the sternum is a cartilaginous one in which the upper five ribs do so by having an actual joint. The lower four ribs (6 to 9) due so by a direct cartilage junction to the bone. At the lower end of the sternum these rib attachments can be at an angle based on the shape of the sternum. That can lead to a prominence of this junction or bumps.
The xiphoid process at the lower end of the sternum is a pointed cartilage structure that has numerous variations in its shape and angulations from the sternum. It is a source of numerous muscular attachments including the rectus abdominus as well as the pericardial sac. It often becomes calcified later in life but can still maintain a joint-like articulation with the sternum. Its most inferior end can be angled outward creating a prominent midline bump below the sternum.
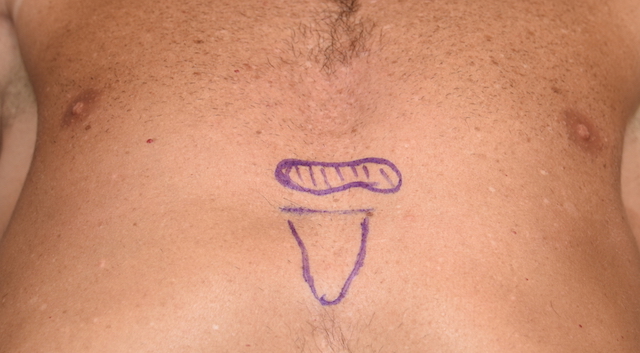
 Case Study: This male patient was bothered by the appearance of his lower sternal area. There were two prominent bumps at the side of the sternum which were connected by a raised line between them. More inferiorly the end of the xiphoid process was prominent.
Case Study: This male patient was bothered by the appearance of his lower sternal area. There were two prominent bumps at the side of the sternum which were connected by a raised line between them. More inferiorly the end of the xiphoid process was prominent.

 Under general anesthesia and through a 3 cm horizontal skin incision, the two lower lateral sternal bumps were exposed and revealed to be cartilage in nature. That were at the articulation points of the 7th ribs to the sternum. They were reduced by shaving them down. The horizontal connection between them was seen to be bone of the sternum and was drilled down by high speed burring.
Under general anesthesia and through a 3 cm horizontal skin incision, the two lower lateral sternal bumps were exposed and revealed to be cartilage in nature. That were at the articulation points of the 7th ribs to the sternum. They were reduced by shaving them down. The horizontal connection between them was seen to be bone of the sternum and was drilled down by high speed burring.
 The xiphoid process was exposed and seen to be all cartilage which was very mobile. It was freed up from its soft tissue attachments and removed. (xiphoidectomy) This exposed the underlying epigastric fat which was closed over by the posterior sheath of the rectus muscle and the muscle themselves by suturing the two sides.
The xiphoid process was exposed and seen to be all cartilage which was very mobile. It was freed up from its soft tissue attachments and removed. (xiphoidectomy) This exposed the underlying epigastric fat which was closed over by the posterior sheath of the rectus muscle and the muscle themselves by suturing the two sides.
 Reshaping of the lower sternal involves reduction of any cartilage or bone prominences. A prominent diploid process can be removed. This can be done directly by a small overlying skin incision that will heal in an almost inconspicuous manner.
Reshaping of the lower sternal involves reduction of any cartilage or bone prominences. A prominent diploid process can be removed. This can be done directly by a small overlying skin incision that will heal in an almost inconspicuous manner.
Case Highlights:
1) The shape of the lower sternum into the upper abdomen ideally should have a valley-like contour between the pectoralis and rectus abdominus muscles
2) Protrusions along the sternum can be due to cartilage prominences from the articulation with the ribs.
3) An outwardly angled xiphoid process can create a protrusion at the lower end of the sternum/upper abominal area.
4) Through a small horizontal skin incision the lower end of the sternum can be reshaped and the xiphoid process removed.
Dr. Barry Eppley
Indianapolis, Indiana