

Background: Clavicle lengthening is one type of shoulder reshaping surgery with the intent of creating a more masculine upper torso appearance. While increased shoulder width is one of the desired effects, changing a rounded shape to a more square or angular shoulder appearance is equally important. Small clavicle lengths create rounder shoulders with a more obtuse angle while a longer clavicle length creates a shoulder with a less obtuse angle that appears less round.
There are two basic methods to lengthen the clavicle, an interpositional bone graft and an osteotomy technique. Each has their advantages and disadvantages. An interpositional bone graft provides a strong wedge between two blunt cut clavicle bone ends and has the ability to maximally length the bone to 2.5cms per side as a result. Its disadvantage is that it requires a fibular bone graft harvest and will take longer to form a solid bony consolidation. Conversely the osteotomy technique does not require a bone graft and has the potential to heal more rapidly. dependent on the type of osteotomy technique used. But it creates less lengthening as the push to separate the two cut ends of the bone is less.
The osteotomy technique for clavicle lengthening is far from an established technique. But borrowing from the sagittal split osteotomy technique for the mandible, known as the SSRO, the concept of maintaining normal bone thickness/contour in the central aspect of where the bone is lengthened makes good biologic sense. This allows for more rapid healing, and combined with plate and screw fixation, should allow adequate bone healing to have occurred in 6 weeks after the surgery.

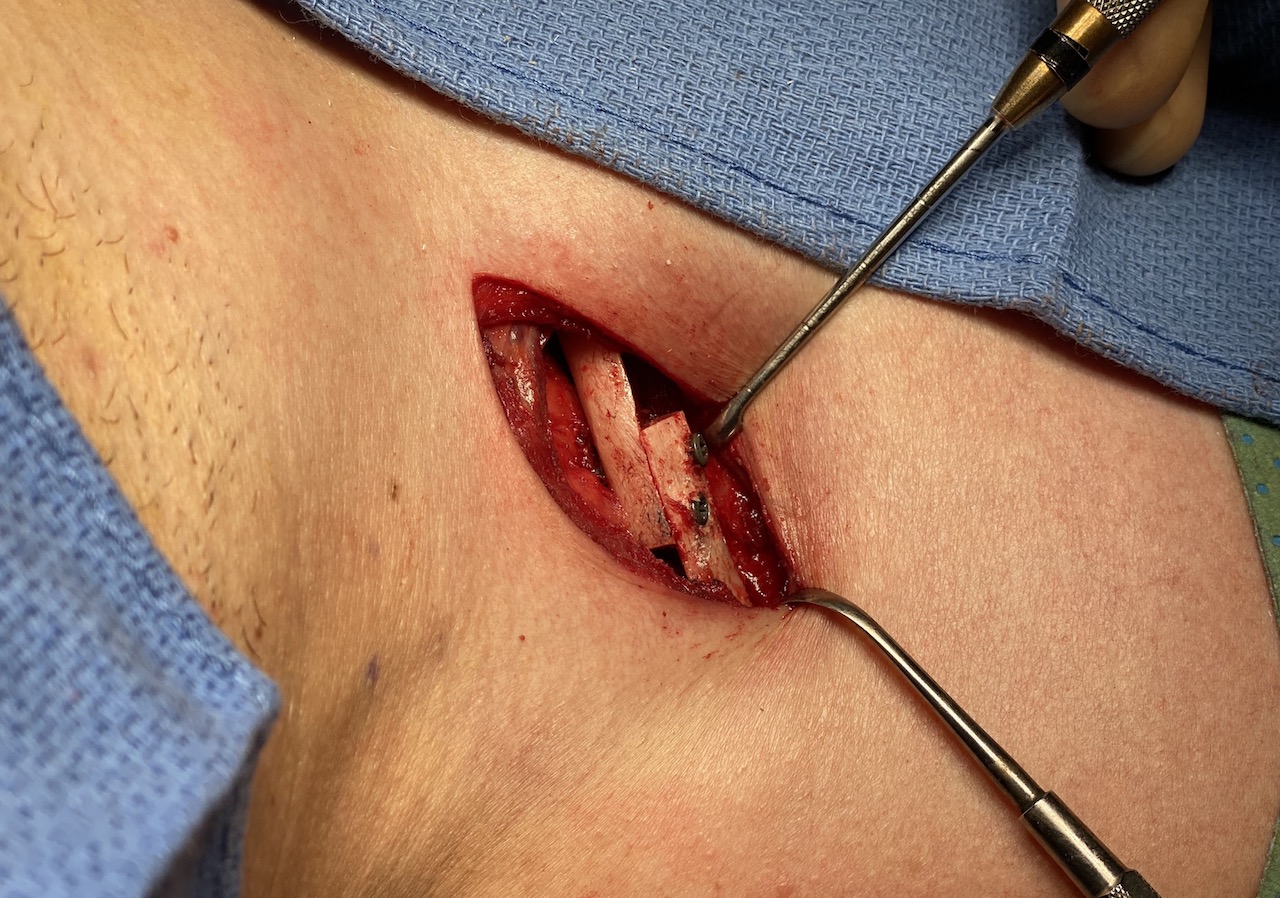
 Case Study: This male desired to have wider and less round-shaped shoulders. He did not have any visible clavicle show. Under general anesthesia and through 4 cm supraclavicular fossa incisions the clavicle was exposed circumferentially at the incision site and on its superior surface from joint to joint. (sternoclavicular joint medially and acromioclavicular joint laterally) A midline sagittal split osteotomy was marked with 90 degree partial thickness bone cuts at opposite sides of the midline mark. A reciprocating saw made all three cuts, preserving the inferior cortex of the full thickness sagittal cut until last.
Case Study: This male desired to have wider and less round-shaped shoulders. He did not have any visible clavicle show. Under general anesthesia and through 4 cm supraclavicular fossa incisions the clavicle was exposed circumferentially at the incision site and on its superior surface from joint to joint. (sternoclavicular joint medially and acromioclavicular joint laterally) A midline sagittal split osteotomy was marked with 90 degree partial thickness bone cuts at opposite sides of the midline mark. A reciprocating saw made all three cuts, preserving the inferior cortex of the full thickness sagittal cut until last.

 Once the bone cuts were complete the sagittal split osteotomy separated easily. The shoulder was pulled outward as much as possible (aided by a midline back roll placed vertically down the spine before draping) and the clavicle lengthened along the split as much as possible. (lengthening the clavicle is not as easily done as shortening it) With considerable effort in this patient 20mm was achieved on the right and 18mms on the left.
Once the bone cuts were complete the sagittal split osteotomy separated easily. The shoulder was pulled outward as much as possible (aided by a midline back roll placed vertically down the spine before draping) and the clavicle lengthened along the split as much as possible. (lengthening the clavicle is not as easily done as shortening it) With considerable effort in this patient 20mm was achieved on the right and 18mms on the left.

 The sagittal split bone was then clamped together and secured with lag screws to hold it together and to stabilize the length. A 10 hope clavicle trauma plate was bent and applied with 3 or 4 bicortical screws on the medial side of the sagittal split area.
The sagittal split bone was then clamped together and secured with lag screws to hold it together and to stabilize the length. A 10 hope clavicle trauma plate was bent and applied with 3 or 4 bicortical screws on the medial side of the sagittal split area.

 On the outer aspect of the clavicle from the sagittal split site three bicortical screws were placed into the plate holes using a small 5mm incision and a drill guide. Unlike the medial plate holes, the lateral plate holes are not accessible from the incision through which the osteotomy is performed.
On the outer aspect of the clavicle from the sagittal split site three bicortical screws were placed into the plate holes using a small 5mm incision and a drill guide. Unlike the medial plate holes, the lateral plate holes are not accessible from the incision through which the osteotomy is performed.

 Lastly 5cc of allogeneic bone putty was applied into the two partial thickness bone defects from the split osteotomy and shaped into a tubular bone shape. The incisions were then closed in multiple layers over a drain on each side.
Lastly 5cc of allogeneic bone putty was applied into the two partial thickness bone defects from the split osteotomy and shaped into a tubular bone shape. The incisions were then closed in multiple layers over a drain on each side.
Before and immediate clavicle lengthening changes.


 While lengthening the clavicle (shoulder widening) seems to be the exact opposite of clavicle shortening (shoulder narrowing) there are several aspects of it that are quite different. The obvious one is how to create bone to make it longer. The true sagittal split technique accomplishes this without needing a bone graft or requiring a prolonged recovery period of months for adequate bone healing. The created bone gap is split between the two sides of the expanded clavicle, maintaining a central 1cm area of full thickness bone. This is critical in allowing rapid bone healing. The bone defect is converted into two partial thickness defects on opposite sides of the bone split which is filled in with bone putty.
While lengthening the clavicle (shoulder widening) seems to be the exact opposite of clavicle shortening (shoulder narrowing) there are several aspects of it that are quite different. The obvious one is how to create bone to make it longer. The true sagittal split technique accomplishes this without needing a bone graft or requiring a prolonged recovery period of months for adequate bone healing. The created bone gap is split between the two sides of the expanded clavicle, maintaining a central 1cm area of full thickness bone. This is critical in allowing rapid bone healing. The bone defect is converted into two partial thickness defects on opposite sides of the bone split which is filled in with bone putty.
While the bone split technique is very different from the two blunt cut ends that come together in clavicle reduction, the really significant clinical difference is in how much harder it is to expand the bone than it is to collapse it inward in reductions. The bony humerus and scapula with their soft tissue attachments provide substantial restrictions in pushing the freed clavicle segment outward. Despite every intraoperative maneuver it is difficult to get any patient past 20mms of lengthening. For this reason I would advise all clavicle lengthening patients to undertake shoulder stretching/expansion therapy prior to surgery to help overcome some of these anatomic restrictions.
Case Highlights:
1) Clavicle lengthening is one type of masculine shoulder augmentation.
2) The sagittal split osteotomy technique offers a method of maintaining maximal bone contact and thickness as the clavicle is lengthened.
3) Allogeneic bone putty fills in the split thickness bone defects to expedite healing and restore normal bone thickness.
4) The amount of clavicle lengthening possible is influenced by the limitation of the shoulder soft tissues which can be aided by a preoperative stretching regimen.
Dr. Barry Eppley
Indianapolis, Indiana