

Background: Facial reshaping surgery most commonly involves modifications of the bones albeit augmentative or reductive. Masculinizing the face is typically augmentative in nature while facial feminization focuses mainly on reduction procedures. It is for this reason that facial masculinization almost always involves implants with a few exceptions such as the sliding genioplasty for chin augmentation and more rarely zygomatic widening osteotomies.
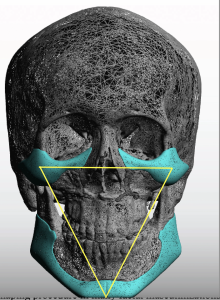
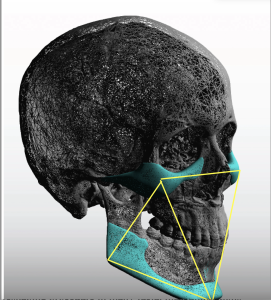 The combination of cheek and jaw implants is the most common facial reshaping procedure in many facial masculinizations because of its five corner (cheek, chin and jaw angles) augmentation effects. There is also the triangulation effects of the corner augmentations which is aesthetically beneficial in creating improved facial definition.
The combination of cheek and jaw implants is the most common facial reshaping procedure in many facial masculinizations because of its five corner (cheek, chin and jaw angles) augmentation effects. There is also the triangulation effects of the corner augmentations which is aesthetically beneficial in creating improved facial definition.
In thicker facial tissue patients, often seen in rounder for fuller faced patients, there is a limit as to how much facial definition can be achieved. It is true that the greater the corner augmentations the more the soft tissues are stretched out over the augmentation and what lies between them (trampoline area) becomes less full. This is where defatting in the non-skeletally supported areas (cheeks and neck) may help collapse the soft tissue between the augmentations. But there is a balance between too much of an augmentation in trying to achieve that effect. While improved facial definition is always a good goal in the thick skinned patient improved facial proportions may be the more realistic goal.
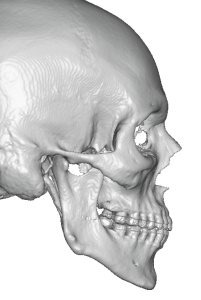 Case Study: This male desired cheek and jaw implants to improve his his facial shape. His 3D CT scan showed a classic high jaw angle appearance with a steep mandibular plane angle. Often in the high jaw angled male there are strong masseter muscle ligamentous attachments. He has no undereye concerns and his desired cheek augmentation was modest in amount. He felt that buccal fat removal below the cheek augmentation would enhance the cheek definition and keep the cheeks from becoming too big particularly when smiling.
Case Study: This male desired cheek and jaw implants to improve his his facial shape. His 3D CT scan showed a classic high jaw angle appearance with a steep mandibular plane angle. Often in the high jaw angled male there are strong masseter muscle ligamentous attachments. He has no undereye concerns and his desired cheek augmentation was modest in amount. He felt that buccal fat removal below the cheek augmentation would enhance the cheek definition and keep the cheeks from becoming too big particularly when smiling.
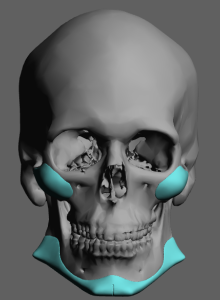
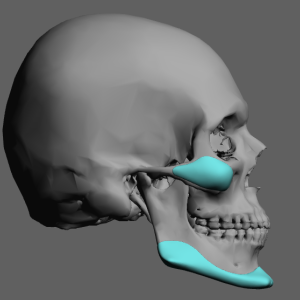
 Using his 3D CT scan custom cheek and jaw angle implants were designed to address his augmentation needs….significant chin augmentation (8mm horizontal), a modest vertical jaw angle lowering (4mms), significant jaw angle widening (10mm) and a linear connection between the chin and jaw angles. The cheek implants were of a high cheekbone shape with 4mms projection and extended arch extension. No infraorbital extension was needed.
Using his 3D CT scan custom cheek and jaw angle implants were designed to address his augmentation needs….significant chin augmentation (8mm horizontal), a modest vertical jaw angle lowering (4mms), significant jaw angle widening (10mm) and a linear connection between the chin and jaw angles. The cheek implants were of a high cheekbone shape with 4mms projection and extended arch extension. No infraorbital extension was needed.
 The forward chin movement and the lowering of his jaw angles decreased his mandibular plane angle.
The forward chin movement and the lowering of his jaw angles decreased his mandibular plane angle.
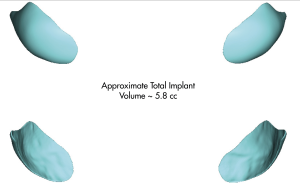
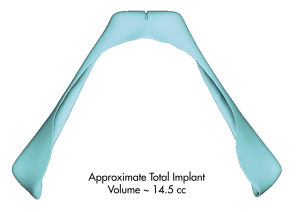 Patients usually only focus on the linear changes at the chin and jaw angle areas, which is understandable, but often overlooked is their volumetric displacement effect. This is an important consideration in large surface area facial implants as it gives one a feel for what the size increase effect may be. Each cheek implants was approximately 3ccs while the jawline implant was about 15ccs.
Patients usually only focus on the linear changes at the chin and jaw angle areas, which is understandable, but often overlooked is their volumetric displacement effect. This is an important consideration in large surface area facial implants as it gives one a feel for what the size increase effect may be. Each cheek implants was approximately 3ccs while the jawline implant was about 15ccs.

 Under general anesthesia the custom jawline implant was placed through the traditional three incisional approach while the cheek implants were placed intraorally.
Under general anesthesia the custom jawline implant was placed through the traditional three incisional approach while the cheek implants were placed intraorally.
 Buccal lipectomies were also performed with the cheek implants and a direct submental lipectomy was performed through an open approach.
Buccal lipectomies were also performed with the cheek implants and a direct submental lipectomy was performed through an open approach.


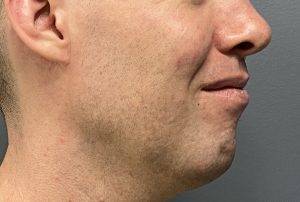
 He went on to uncomplicated healing and one year later his results improved facial proportions. I don’t think he achieved great facial definition bit his thick tissues made that never a realistic obtainable result. Select areas of facial defatting helps somewhat and are usually worthwhile ancillary procedures in many facial augmentation patients with thicker tissues.
He went on to uncomplicated healing and one year later his results improved facial proportions. I don’t think he achieved great facial definition bit his thick tissues made that never a realistic obtainable result. Select areas of facial defatting helps somewhat and are usually worthwhile ancillary procedures in many facial augmentation patients with thicker tissues.
Key Points
1) The combination of custom cheek and jawline implants is the common structural facial reshaping procedure for men.
2) In thicker skin/tissue patients fat reduction in the bony supported trampoline area is often done as well to help with enhancing whatever facial definition is possible to achieve.
3) Thick tissue patients present challenges for obtaining as much facial definition as they would like but they do always obtain better facial proportions.
Dr. Barry Eppley
World-Renowned Plastic Surgeon