

Background: Cheek implants have been around for over four decades and have undergone some significant evolution in their shapes and cheek augmentation effects. With three basic implant styles (malar, submalar and combined malar-submalar) and numerous sizes between them many different types of cheek augmentation needs can be met.
But what all of these cheek implants have in common in that they provide more oval-shaped augmentation over the prominence of the zygomatic body or cheek bone proper. This area creates the classic fullness that is often desired by women but much less often by men. This suggests that many cheek implant styles, although not their intended objective, are not really gender neutral. Rather there is a significant unintentional gender bias. A rounder or fuller apple of the cheeks enhancement is a feminine aesthetic goal not a male one typically.
Males are typically interested in a more angular or defined cheek look. Which dimensionally means it does not have an oval shape but a more linear line of augmentation. A line is more defined than a circle. Whether this line of augmentation starts a bit lower in the anterior cheek and sweep back across the zygomatic arch or starts higher close to the infraorbital rim level depends on the flavor the high cheekbone look the patient wants.
I have seen numerous male cheek augmentation patients, young and older, that are dissatisfied with their results from standard cheek implants. Improvement is not going to come from repositioning the existing implants or changing size although that may help some of them. Real improvement is going to come from changing the implant style or shape.
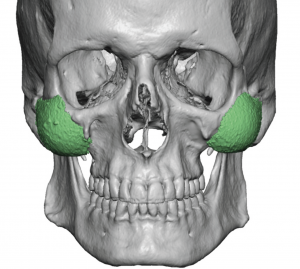
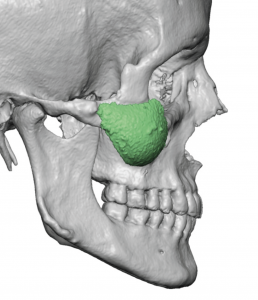 Case Study: This male had standard malar shell cheek implants intraorally several years previously. While he had symmetric placement of the implant as seen on a 3D CT scan, he did not like the apple cheek effect they created.
Case Study: This male had standard malar shell cheek implants intraorally several years previously. While he had symmetric placement of the implant as seen on a 3D CT scan, he did not like the apple cheek effect they created.
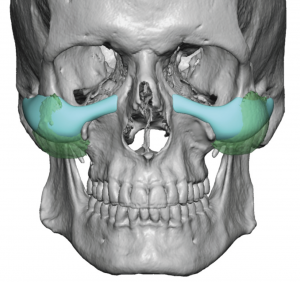
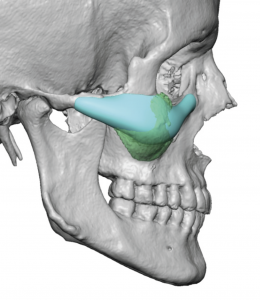
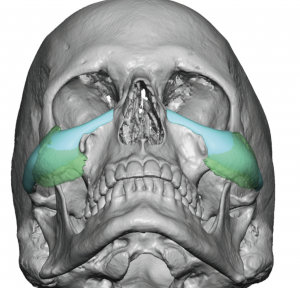
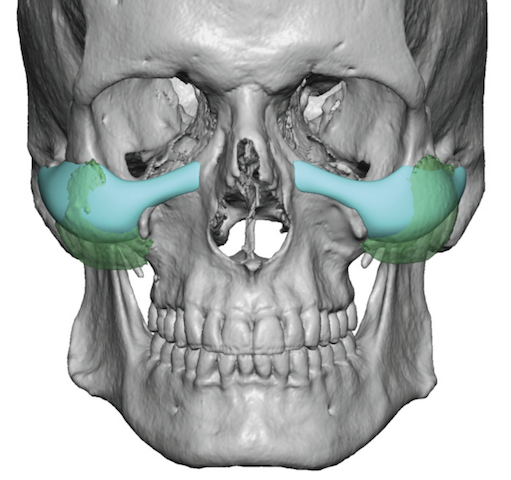
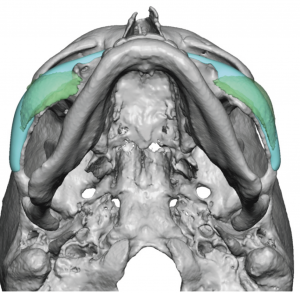 New custom infraorbital-malar implants were designed to create a higher and more defined cheek bone look. Infraorbital extensions were added to address undereye hollowing with arch extensions back towards the temporal process. The new design was overlaid over the existing implants to precisely determine how to create a different cheek augmentation effect.
New custom infraorbital-malar implants were designed to create a higher and more defined cheek bone look. Infraorbital extensions were added to address undereye hollowing with arch extensions back towards the temporal process. The new design was overlaid over the existing implants to precisely determine how to create a different cheek augmentation effect.

 Under general anesthesia and through lower eyelid incisions, the existing cheek implants were removed and new pockets for the increased surface area of the custom implants made. When laid side to side the shape and volumetric differences between the two type of implants could be appreciated.
Under general anesthesia and through lower eyelid incisions, the existing cheek implants were removed and new pockets for the increased surface area of the custom implants made. When laid side to side the shape and volumetric differences between the two type of implants could be appreciated.
 The new custom infraorbital-malar implants were then inserted, positioned and secured with two microscrews per side. The cheek tissues and orbicularis muscle was resuspended and the incisions closed.
The new custom infraorbital-malar implants were then inserted, positioned and secured with two microscrews per side. The cheek tissues and orbicularis muscle was resuspended and the incisions closed.
 For the male cheek implant patient who seeks a specific defined shape result, currently a custom design approach has to be taken. There are two basic custom cheek implant designs, malar and infraornital-malar. The extent of the infraorbital segment determines whether the advised incisional approach is either intraoral or through the lower eyelid.
For the male cheek implant patient who seeks a specific defined shape result, currently a custom design approach has to be taken. There are two basic custom cheek implant designs, malar and infraornital-malar. The extent of the infraorbital segment determines whether the advised incisional approach is either intraoral or through the lower eyelid.
Case Highlights:
1) Some men will not do aesthetically well with standard cheek implants as the fullness is in the wrong anatomic position and has the wrong shape.
2) The high cheekbone look requires a custom implant approach to create as more linear line of augmentation back across the zygomatic arch.
3) The lower eyelid approach can be used to both remove the indwelling cheek implants and place the new custom cheek implants.
Dr. Barry Eppley
Indianapolis, Indiana