


Background: Aesthetic augmentation of the cheek area is second only in frequency to that of the chin and jawline. But unlike the lower third of the face the term ‘cheek’ is imprecise when defining what a patient wants to accomplish and there are significant gender differences in what this term means. As the cheek area is connected to the orbital and upper jaw bones these neighboring structures may comprise part of what the patient sees or desires to augment.
Contemporary facial implant design technology has brought a paradigm shift in understanding and achieving aesthetic cheek augmentation effects. The most popular custom facial implant for the midface today is the infraorbitar-malar (IOM) implant. While there is a standard facial implant that is somewhat similar (extended tear trough implant) its effects are a very distant cousin to what the custom IOM implant can accomplish. Simultaneously augmenting the undereye and cheek areas through a wrap around design the custom IOM can provide profound aesthetic effects. Because of their anatomic connection undereye hollowing and cheek deficiencies are the result of the same anatomic problem and only the IOM implant can satisfactorily address both when a significant deficiency exists.
Once unique feature of the upper midface around the undereye and cheek is its ease of visualization and, as a result, the sensitivity to its aesthetic effects. While the phrase ‘every mlllimeter counts in the face’ is frequently said, that actually is not true in all facial areas. But in the periorbital-cheek area it is so custom designing is a delicate balance between getting the most aesthetic effect vs risking an overcorrection…which is always a near 100% risk of a revisional surgery being needed.
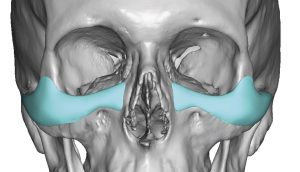
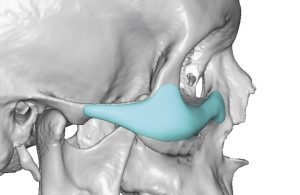 Case Study: This male desired infraorbital-malar augmentation. Careful analysis of his face showed these these deficiencies were moderate in magnitude and a custom IOM implant design was done with a maximum of 4mm projection at the turn of the curve. (infraorbital-malar transition zone)
Case Study: This male desired infraorbital-malar augmentation. Careful analysis of his face showed these these deficiencies were moderate in magnitude and a custom IOM implant design was done with a maximum of 4mm projection at the turn of the curve. (infraorbital-malar transition zone)

 Surgical placement of the custom IOM implants were done through a hemi- lower eyelid incision with screw fixation.
Surgical placement of the custom IOM implants were done through a hemi- lower eyelid incision with screw fixation.


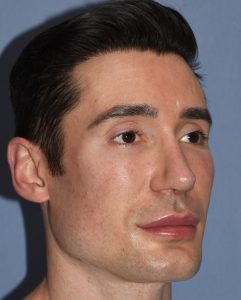
 While he had an uncomplicated recovery and after the tissues had settled into place he felt that it was a bit too heavy/full under the eyes. As a result he desired a revision where the infraorbital component was removed and only a high cheek implant location was maintained.
While he had an uncomplicated recovery and after the tissues had settled into place he felt that it was a bit too heavy/full under the eyes. As a result he desired a revision where the infraorbital component was removed and only a high cheek implant location was maintained.
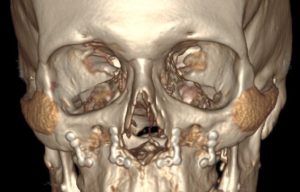
 This revision was done secondarily with a more satisfactory outcome through the lower eyelid incisions. A 3D CT scans showed the new shape and position of the modified IOM implants.
This revision was done secondarily with a more satisfactory outcome through the lower eyelid incisions. A 3D CT scans showed the new shape and position of the modified IOM implants.
Any facial implant, including custom facial implant designs, are prone to a relatively high rate of revisional surgery for implant modification or for new implants entirely. No one can predict with absolute accuracy their aesthetic effects, or equally importantly, how the patient will feel about the result. While implants can be placed properly and heal beautifully with no adverse consequences that is not an assurance that the aesthetic outcome will be equally achieved. The periorbital-cheek areas is much like the nose in that a millimerte or two of change can swing the balance between a good aesthetic result and one the patient wants to change. This is especially true in the patient with more modest aesthetic deficiencies as the acceptable target zone is much smaller than in bigger aesthetic concerns.
Key Points:
1) The undereye/cheek area is an exquisitely sensitive area for augmentation in terms of its aesthetic effects.
2) The high cheek implant may or may not include an infraorbital component based on patient preference and tolerance for change.
3) Revision of custom infraorbital-malar implants is not rare for either projection or footprint reduction or both.
Dr. Barry Eppley
World-Renowned Plastic Surgeon