

Background: Cheek implants have been around for nearly fifty years and their basic styles have largely remained the same. Malar, submalar and combinations thereof (aka shell implants) have been the mainstay of implant-based cheek augmentation which can be effective for many patients. In an otherwise normal volume face these implants work best in women and not men as enhanced submalar volume can feminize the male face. This generally explains the not uncommon lack of aesthetic success with the use of standard cheek implants for many surgeons.
But in the male face that has loss of submalar volume or a thinner and more bony appearance (gaunt) the addition of volume in the anteroinferrior cheek area can be of aesthetic benefit. In men that have sustained such improvement with standard cheek implants there is also the question of implant placement…what is the actual position of the implant on the bone that has resulted in the favorable effect. This becomes relevant if the patient needs the cheek implants replaced …regardless of the reason.
A certain percentage of cheek implant patients may still seek injectable filler treatments afterwards if they desire additional volume. While these are usually successful there is always the rare chance of inducing an implant infection should the needle inadvertently enter the implant capsule. While the use of oral antibiotics may temporarily suppress the infection it is rare that antibiotics alone can cure it. Almost always the infected cheek implant will need to be removed. With unilateral cheek implant removal how it is replaced depends on how satisfied the patient was with the result before the infection. By getting injectable fillers the concept of making larger custom cheek implant replacements becomes relevant. This desire is magnified if cheek implant asymmetry was also present previously.
 Case Study: This male had indwelling standard cheek implants of which the left side became infected after an injectable filler treatment five years after the surgery. He was treated with oral antibiotics which suppressed it but the swelling never fully sent down. He decried to have both cheek implants removed, design new custom cheek implants and place them 3 to 4 months later. His 3D Ct scan showed the cheek implants prior to their removal which were a large submalar style screwed to the bone. There was implant asymmetry due to underlying bony asymmetry.
Case Study: This male had indwelling standard cheek implants of which the left side became infected after an injectable filler treatment five years after the surgery. He was treated with oral antibiotics which suppressed it but the swelling never fully sent down. He decried to have both cheek implants removed, design new custom cheek implants and place them 3 to 4 months later. His 3D Ct scan showed the cheek implants prior to their removal which were a large submalar style screwed to the bone. There was implant asymmetry due to underlying bony asymmetry.
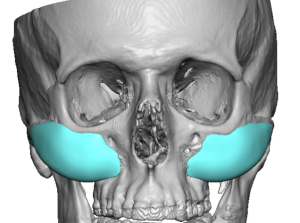
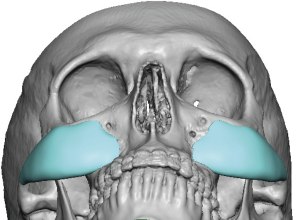
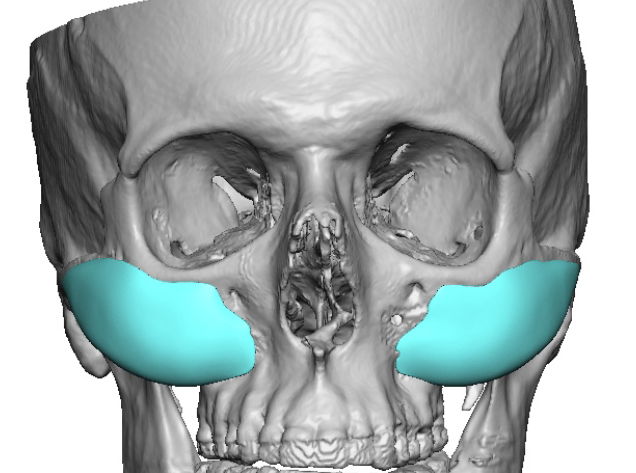
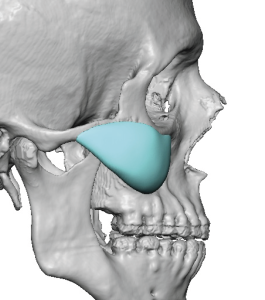 Based on the shape of his existing submalar cheek implants and that at least 2ccs of filler was regularly added (more on the right than the left), new custom cheek implants were designed. The custom implant volumes were 8ccs on the right and 7ccs on the left.
Based on the shape of his existing submalar cheek implants and that at least 2ccs of filler was regularly added (more on the right than the left), new custom cheek implants were designed. The custom implant volumes were 8ccs on the right and 7ccs on the left.
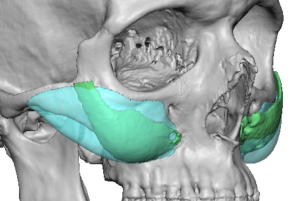
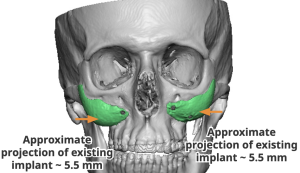
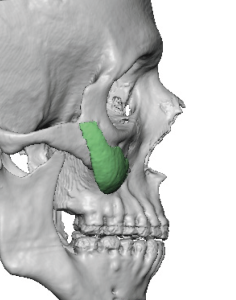
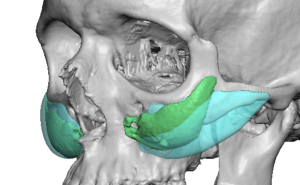 The best way to view the differences between the standard vs the new custom implant designs is seen in the oblique overlays.
The best way to view the differences between the standard vs the new custom implant designs is seen in the oblique overlays.

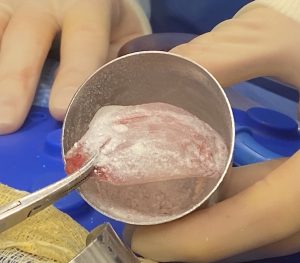 While the custom cheek implants were being designed and made the standard cheek implants were removed. Four months later the new custom cheek implants were inserted through the original intraoral incisions. Besides using screw fixation the implants were prepared prior ti insertion with 4mm perfusion holes placed by a dermal punch. Besides allowing soft tissue ingrowth after surgery they also permit the holes to be filled with antibiotic powder…an extra step in the previous infected implant patient.
While the custom cheek implants were being designed and made the standard cheek implants were removed. Four months later the new custom cheek implants were inserted through the original intraoral incisions. Besides using screw fixation the implants were prepared prior ti insertion with 4mm perfusion holes placed by a dermal punch. Besides allowing soft tissue ingrowth after surgery they also permit the holes to be filled with antibiotic powder…an extra step in the previous infected implant patient.

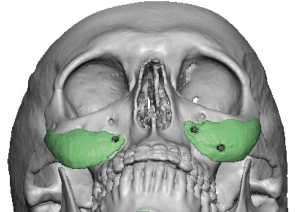
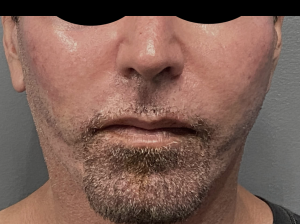 The immediate change in the submalar facial appearance could be appreciated with a doubling of the cheek implant coverage area as well as the footprint of the implant.
The immediate change in the submalar facial appearance could be appreciated with a doubling of the cheek implant coverage area as well as the footprint of the implant.
The first pair of cheek implants provides invaluable information about how to custom design new ones, particularly if their effect is in the correct dimensional type of change. This type of desired cheek augmentation effect is uncommon in men with the exception if submalar hollowing or a deficiency exists. While the first set of implants in this case produced a positive effect with enhanced submalar fullness and the patient kept the initial result for years, an implant infection prompted the desire for an increased volume change.
Key Points:
1) The first set of standard cheek implants provides invaluable insight in how to make a new custom cheek implant design better…particularly if fillers have been added them secondarily.
2) Most standard cheek implants will not work for many men but when submalar hollows are present the concept becomes more effective.
3) Cheek asymmetry is rarely satisfactorily improved with the use of standard implants as it is nearly impossible to ‘eyeball’ the differences with implants.
Dr. Barry Eppley
World-Renowned Plastic Surgeon