

Background: Skin laxity is a common anatomic result of aging which affects body areas differently. The greatest amount of age-related skin excesses typically occur in joints in the extremities, most notably the elbows and knees. These extremity areas are continuously flexed and extended often well beyond 90 degrees for extended time periods over a lifetime. As a result it is inevitable that multiple folds of skin will be the result.
The skin across bony prominences of the elbow and knees by design has to be flexible and supple to not impede joint motion. But decades of motion across these extremity joints will create considerable skin excesses that is fully seen in arm and leg extension. These skin excesses are seen on the front of the knees and on the back of the arm at the elbows.
These skin excesses can be an aesthetic concern to some people and their reduction may be desired. Like skin excesses anywhere on the body excision of part or all of them can be done with the tradeoff of a scar. But unlike many other more typical aesthetic skin excision procedure excess skin removal across a movable joint poses a unique set of surgical considerations. Such excisions must take into account the effect of the excision when the extremity is fully flexed as this can affect healing and ultimately potential widening of the scar.

 Case Study: This older male was bothered by the skin folds at his elbows which was maximally seen with the arms extended. He had a fair complexion and his skin was known to be notoriously dry.
Case Study: This older male was bothered by the skin folds at his elbows which was maximally seen with the arms extended. He had a fair complexion and his skin was known to be notoriously dry.

 Markings for elbow lifts were done initially with the arm extended using a crescent-shaped excision pattern with the lower end being just above the elbow point. The amount of excision was then checked with the arm bent at 90 degrees. Checking in the bent arm position allows for adjustments to be made. The goal is to have the final line of closure and the eventual scar above the elbow point to prevent scar widening.
Markings for elbow lifts were done initially with the arm extended using a crescent-shaped excision pattern with the lower end being just above the elbow point. The amount of excision was then checked with the arm bent at 90 degrees. Checking in the bent arm position allows for adjustments to be made. The goal is to have the final line of closure and the eventual scar above the elbow point to prevent scar widening.

 Under local anesthesia and in the prone position with the arms bent over an arm board to provide direct access to the elbows, the skin markings were incised and the intervening skin removed.
Under local anesthesia and in the prone position with the arms bent over an arm board to provide direct access to the elbows, the skin markings were incised and the intervening skin removed.
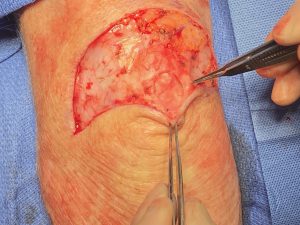
 In both arms a empty bursa sac was encountered over the point of the elbow. (olecranon) The inferior skin flap was advanced up over the olecranon and closed in in a curvilinear fashion on the triceps side of the elbow.
In both arms a empty bursa sac was encountered over the point of the elbow. (olecranon) The inferior skin flap was advanced up over the olecranon and closed in in a curvilinear fashion on the triceps side of the elbow.
The elbow lift is unique as it involves an excision of tissue across a movable joint. This places the closure under tension and a necessity of having the closure line away from the maximal point of tension with arm flexion. Enough excessive skin has to be excised to make the procedure worthwhile but too much tissue removed can create scar widening which may be viewed as aesthetically disturbing as the original problem.
Bursa sacs are a common development at the elbow and are usually fluid-filled, serving as a smooth gliding cushion between a bone surface and the overlying tissues. While some are congenital in origin most develop over time due to friction. While some develop inflammation and become infected (bursitis), many remain quiescent and are unknown to the patient. Such was the case in this patient where the bursa sac was empty and thin. There is no need to remove the entire bursa lining as it does have a biologic purpose of making a gliding surface over the elbow joint.
Key Points:
1) Skin laxity is a common sequelae of aging across a movable joint like the elbow.
2) Elbow skin laxity can be treated by excision and lift if the resultant scar is considered a fair aesthetic tradeoff.
3) In elbow lifts bursa cavities can occasionally be encountered during the excision.
Dr. Barry Eppley
World-Renowned Plastic Surgeon