

Background: The sternum is the long flat bone running down the middle of the chest, serving as attachments for the clavicles and ribs. It typically has a convex outer surface as it descends inferiorly, becoming more narrow at its lowest point where it articulates with the xiploid process, sometimes referred to as the ensiform process. (both words mean ‘swordlike’)
The xiphoid process is a cartilaginous extension from the lower end of the sternum, is pointed in shape and typically angles downward. It is usually felt as a lump just below the sternal notch.While it has a fibrous joint attachment with the lower end of the sternum this is a non-movable joint. The xiploid process will go on to ossify after the age of 40. Its functional role is that it serves as a site of numerous muscle attachments including the rectus abdominus and the diaphragm.

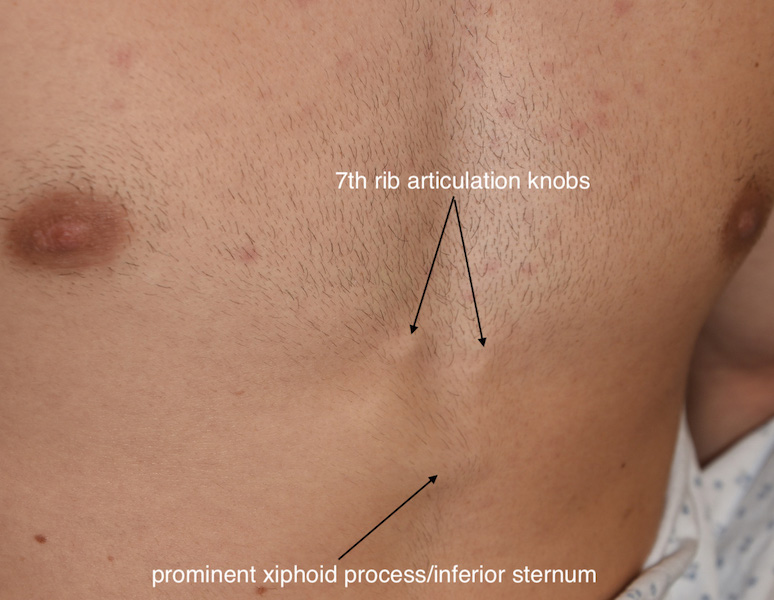
 Despite its simplicity of structure the xiphoid process has numerous anatomic variations from bifurcations to perforations. But one of the more common is how it can become angulated outward, creating a prominent end with an inward valley above it. Often associated with this xiphoid process protrusion are prominent articulations of the 7th ribs at the inferior angle of the sternum which appear as a pair of bumps. When put together these three protrusions are seen separated by a valley between them.
Despite its simplicity of structure the xiphoid process has numerous anatomic variations from bifurcations to perforations. But one of the more common is how it can become angulated outward, creating a prominent end with an inward valley above it. Often associated with this xiphoid process protrusion are prominent articulations of the 7th ribs at the inferior angle of the sternum which appear as a pair of bumps. When put together these three protrusions are seen separated by a valley between them.
While there are no functional issues to this type of inferior sternal/upper abdominal protrusions, it can be a source of aesthetic distraction to those affected. They are usually most evident the leaner a patient is as the hard structures become more evident with little subcutaneous fat thickness.
Case Study: This young fit male had been bothered since he was a teenager with the appearance of his lower sternal area. He had the triangulated appearance of bilateral 7th rib articulation humps with an upwardly angled xiphoid process.

 Under general anesthesia and through a small 3 cm horizontal incision the 7th rib bumps were shaved down.
Under general anesthesia and through a small 3 cm horizontal incision the 7th rib bumps were shaved down.

 Dissection down to the end of the sternum revealed a small cartilaginous end of the xiphoid process which was removed. It became apparent that the outward deflection was not predominantly the usual cartilaginous xiphoid process but a very calcified/ossified xiphoid process that was indistinguishable from sternal bone. Using a handpiece and burr the calcified large xiphoid process was burred down to a thin inner layer. It was then carefully separated from the underlying soft tissue attachments and then carefully removed. Further reshaping of the end of the sternum was done to smooth out its edges. (inferior sternoplasty) Prior to skin closure the upper rectus muscle were plicated across the defect.
Dissection down to the end of the sternum revealed a small cartilaginous end of the xiphoid process which was removed. It became apparent that the outward deflection was not predominantly the usual cartilaginous xiphoid process but a very calcified/ossified xiphoid process that was indistinguishable from sternal bone. Using a handpiece and burr the calcified large xiphoid process was burred down to a thin inner layer. It was then carefully separated from the underlying soft tissue attachments and then carefully removed. Further reshaping of the end of the sternum was done to smooth out its edges. (inferior sternoplasty) Prior to skin closure the upper rectus muscle were plicated across the defect.



 His intraoperative results showed the degree of yeti effects of bump reductions and the inferior sternoplasty. When removing the xiphoid process, whether it is completely cartilaginous or bone, it is important to remember that the inferior sternopericardial ligament attaches the pericardium to the posterior xiphoid process as well as being an attachment for the diaphragm.
His intraoperative results showed the degree of yeti effects of bump reductions and the inferior sternoplasty. When removing the xiphoid process, whether it is completely cartilaginous or bone, it is important to remember that the inferior sternopericardial ligament attaches the pericardium to the posterior xiphoid process as well as being an attachment for the diaphragm.
Case Highlights:
1) A xiphoid process prominence is a not uncommon lower sternal aesthetic deformity which can occur in very fit young men.
2) The inferior sternum can also have prominent bumps/knobs which are the 7th rib articulations with the sternum
3) Through a small horizontal incision over the lower sternum the 7th rib bumps and a xiphoidectomy can be performed.
4) In some cases of a prominent angulated xiploid process most of the prominence may be any rather than cartilaginous.
Dr. Barry Eppley
Indianapolis, Indiana