


Background: The mid-body region for contouring can be done by a variety of surgical procedures. The most well known and commonly done are liposuction, fat transfer augmentations and buttock implants. This collection of now standard procedures can satisfy most patient’s needs for a smaller waistline, larger and more shapely buttocks and, in some cases, even hip augmentation.
There are also newer body contouring procedures that are available for more significant or ‘extreme’ changes when the standard procedures are either inadequate to achieve the patient’s goal or the patient desires more of a change than they have already provided. Rib removal surgery can go beyond what liposuction can achieve. Custom buttock implants can be made in sizes that standard implants do not have. Custom hip implants provides a more assured and effective hip augmentation than fat injection grafting.
Combining these newer body contouring procedures in a single surgery provide the greatest amount of trunk contouring possible. But it requires a highly motivated patient to do so and one that also understand the nature of the recovery process as well as the risks and complications of such an unusual collection of procedures.
Case Study: This female desired to have a major body contouring change with as small a waistline as possible, as large a buttock augmentation as her tissues would permit and an assured method to fill in her hip dip areas. She did not have enough to harvest to even come close to her buttock and hip augmentation goals.


 Under general anesthesia in the prone position custom 700cc buttock implants were initially placed in the subfascial pocket through paired paramedic intergluteal incisions. Custom hip implants of 300ccs were placed on top of the TFL fascia in the deep subcutaneous position through a high hip incision. Finally rib removal surgery was done through lateral flank incisions doing a combination of flank liposuction, removal of the outer half of ribs 11 and 12 and removing the outer portion of the latissimus dorsi muscle.
Under general anesthesia in the prone position custom 700cc buttock implants were initially placed in the subfascial pocket through paired paramedic intergluteal incisions. Custom hip implants of 300ccs were placed on top of the TFL fascia in the deep subcutaneous position through a high hip incision. Finally rib removal surgery was done through lateral flank incisions doing a combination of flank liposuction, removal of the outer half of ribs 11 and 12 and removing the outer portion of the latissimus dorsi muscle.





 She recovered without complications from this extensive surgery and was not seen again for several years when she reappeared for a facial procedure. Her results from these combined procedures could then be assessed. She had begin to have some of her tattoos treated for removal as seen on her left hip and thigh.
She recovered without complications from this extensive surgery and was not seen again for several years when she reappeared for a facial procedure. Her results from these combined procedures could then be assessed. She had begin to have some of her tattoos treated for removal as seen on her left hip and thigh.
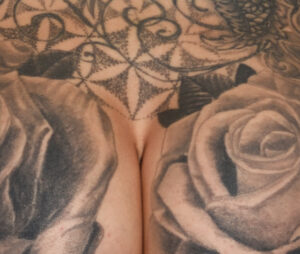


 Visual inspection of her intergluteal, hip and back scars revealed minimal scarring even amidst the tattoo coverage of the back and hip areas.
Visual inspection of her intergluteal, hip and back scars revealed minimal scarring even amidst the tattoo coverage of the back and hip areas.
This extreme type of body contouring surgery merits discussion in terms of both recovery and potential risks and complications. Interestingly one would assume that the major recovery would come from the rib removal part of the surgery. But that is surprisingly not true. I have always been impressed with a lower level of discomfort from rib removal surgery than one would think. It is often compared to recovery from rib fractures but that is not an accurate correlation as there are no bones to heal. Thus it is really about muscle discomfort not bone pain. Much more discomfort comes from the buttock and hip implants even though they do not directly invade the muscles. That being said suffice it to say the combing all three of these procedures does make for a collective challenging recovery.
Similarly one would assume that rib removal surgery would have the highest risk of potential complications. Bit like all autologous vs implant type surgeries, the risks are appreciably higher for implant-related surgeries particularly if they are not placed in or under a muscular place. Seroma collections in particular are a relatively high risk in subfascial buttock and deep subcutaneous hip implants. Postoperative drains are a necessity. But even prolonged use of them does not always ensure they won’t happen. (not using drains is a guarantee that they will happen) Some seromas resolve by aspiration after drainer removal and occasionally some do not. In contrast I have yet to see any fluid collections in rib removal surgery and usually do not use them.
Surprisingly she never experienced any complications during her recovery and went on to have an overall successful aesthetic outcome as seen years later. (she did report at some point after surgery that one of her buttock implants flipped but then it went back into position and has not done so since) But I would not expect such outcomes that from everyone and am not certain that such a collection of body contouring procedures should ever be routinely done when looking at recovery and complication risks.
Case Highlights:
1) Major body contouring changes can be done by the use of uncommon procedures such as custom buttock and hip implants as well as rib removal surgery.
2) Larger buttock implants must be placed in the subfascial pocket if it is a primary procedure. Hip implants can be placed concurrently but its pocket location must not merge with that of the buttock implants.
3) Rib removal can be performed in conjunction with buttock implants in the properly selected patient.