


Background: While standard chin implants are effective for common projection deficiencies, they are not effective for more significant dimensional changes. One reason a chin implant can fail, therefore, is that was a poor selection based on the patient’s anatomic needs/aesthetic goals. In theory this outcome should be largely avoidable using preoperative imaging. But I have seen many patients for chin implant revision that never had any preoperative imaging actually done. (hard to believe but it is actually common)
What constitutes chin augmentation dimensions in which standard chin implants are not effective? The first instance is when any significant vertical increase is needed.(beyond a millimeter to two) Verticality requires either a custom chin implant design or a sliding genioplasty. The second instance is when the horizontal augmentation needed exceeds 10 or 11mms. (larger standard chin implants do not exist) The third instance is when the combined horizontal and vertical increases are needed which collectively exceed the number of 15. While a custom chin implant can be made to a achieve these numbers one must be careful that the soft tissue chin pad can actually stretch over that amount of push from behind. For this reason sliding genioplasties are more effective for significant combined horizontal and vertical augmentation as the soft tissue chin pad remains attached to the front and inferior edge of the bone and therefore remains stretched over it.
One ‘advantage’ of an existing albeit inadequate chin implant is that it provides a dimensional reference. It helps better determine what amount of additional augmentative may be more aesthetically beneficial. This is unlike the first surgery where such dimensional changes are more abstract for the patient.
 Case Study: This male had a prior chin implant procedure using a two-piece Medpor chin implant of 3mms projection placed from a submental incision with four screw fixation. Given his degree of horizontal and vertical chin deficiency the selection of such a small chin implant which could provide no vertical increase is perplexing. Equally perplexing is the common use of large number of screws that are placed in a rigid implant. By simple clinical measurements and computer imaging it was preoperatively determined that 11 or 12mms of total horizontal augmentation was needed as well as 4 or 5mms of vertical increase.
Case Study: This male had a prior chin implant procedure using a two-piece Medpor chin implant of 3mms projection placed from a submental incision with four screw fixation. Given his degree of horizontal and vertical chin deficiency the selection of such a small chin implant which could provide no vertical increase is perplexing. Equally perplexing is the common use of large number of screws that are placed in a rigid implant. By simple clinical measurements and computer imaging it was preoperatively determined that 11 or 12mms of total horizontal augmentation was needed as well as 4 or 5mms of vertical increase.

 Under general anesthesia and through an intraoral approach the Medpor chin implant was identified, unscrewed and removed. Like every Medpor facial implant I have ever seen there is an intervening layer of scar between the implant and the bone. (no bone ingrowth) This underneath layer of scar aids in its removal. It is the outer layer of tissue attachments that is more adherent.
Under general anesthesia and through an intraoral approach the Medpor chin implant was identified, unscrewed and removed. Like every Medpor facial implant I have ever seen there is an intervening layer of scar between the implant and the bone. (no bone ingrowth) This underneath layer of scar aids in its removal. It is the outer layer of tissue attachments that is more adherent.

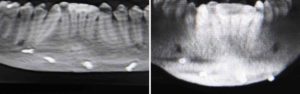
 Then a sliding genioplasty was performed with a 12mm advancement with 5mms of vertical lengthening. The entire bone gap was grafted with 15cc of tissue bank corticocancellous bone chips that had been soaking in an antibiotic solution.
Then a sliding genioplasty was performed with a 12mm advancement with 5mms of vertical lengthening. The entire bone gap was grafted with 15cc of tissue bank corticocancellous bone chips that had been soaking in an antibiotic solution.
Chin implants can aesthetically fail if they are woefully inadequate for the patient’s aesthetic objectives. While largely avoidable with thoughtful preoperative imaging, a sliding genioplasty can be a good replacement particularly when vertical increases are needed. Because of the bony step off deformity created by large sliding genioplasties interpositional corticocancellous chip grafting can be useful to help retire a more normal shape to the chin bone.
Case Highlights:
1) Medpor chin implants are removable and is aided by the capsule which forms between the implant and the bone surface.
2) A sliding genioplasty can create combined horizontal and vertical chin augmentation increases that exceeds what standard chin implants can do.
3) Corticocancellous chip bone grafting can help restore a more natural shape of the chin in large sliding genioplasties.
Dr. Barry Eppley
Indianapolis, Indiana