

Background: Medpor or porous polyethylene is a common facial implant material. Its primary biologic feature as an implant is that is surface porosity permits soft tissue attachments/ingrowth. While this is perceived by some as a material benefit it become a major material liability should any form of revision or removal of the implant be needed. These soft tissue attachments are tenacious and removal can be extremely difficult. Injury to surrounding nerves and blood vessels, if in the vicinity, can be a real risk. The risk of implant removal can be greater than implant insertion which is not a good material feature.
Having removed hundreds of Medpor facial implants none are more challenging than those along the jawline, particularly the jaw angle region. Besides the difficulty working way back in the posterior region of the mouth the soft tissue attachments of the masseter muscle are very adherent. But what really makes this area for Medpor implant removal difficult is that many of the standard jaw angle implants are designed to wrap around the inferior border to create a vertical lengthening effect. While this is a sound design and has good aesthetic benefit it also complicates removal due to the limited intraoral exposure. But one additional variable increases the risk of Medpor jaw angle implant removals…the adherence of the facial artery to the implant as it crosses up from the neck over the implant into the face. I have more than once partially transected this artery during their removals and, while not life threatening, can be difficult to get the bleeding under control.
An alternative approach to Medpor jaw angle implants removal is through a facelift which approaches implant removal from a different and more favorable direction.
 Case Study: This older female had Medpor jaw angle and chin implants placed over 20 years ago. While she liked the chin improvement she never liked the jaw angle augmentation effects as she felt it made her look too masculine. She was going to undergo a facelift and the decision was made to access the implants from this direction and avoid an extensive intraoral dissection and healing period.
Case Study: This older female had Medpor jaw angle and chin implants placed over 20 years ago. While she liked the chin improvement she never liked the jaw angle augmentation effects as she felt it made her look too masculine. She was going to undergo a facelift and the decision was made to access the implants from this direction and avoid an extensive intraoral dissection and healing period.
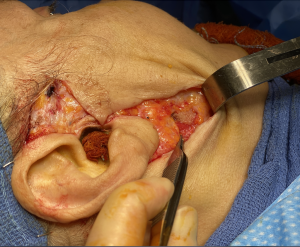
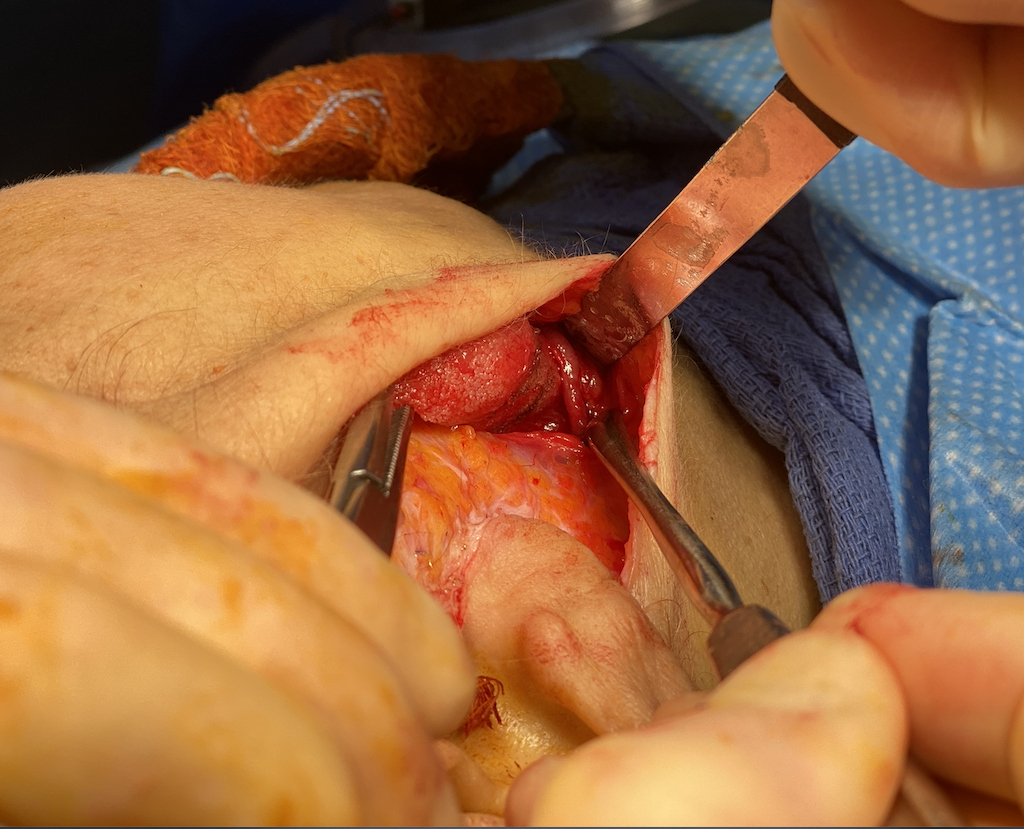
 Under general anesthesia the skin flaps of the facelift were initially raised. Over the posterior jaw angle areas the implants could easily be felt and there did not appear to masseter muscle over the larger back ends of the implants. A small incision was made through the SMAS layer and the implants exposed. The overlying adherent soft tissue attachments were released and the implants elevated off of the bone. A very thick capsule was found around the implant as expected.
Under general anesthesia the skin flaps of the facelift were initially raised. Over the posterior jaw angle areas the implants could easily be felt and there did not appear to masseter muscle over the larger back ends of the implants. A small incision was made through the SMAS layer and the implants exposed. The overlying adherent soft tissue attachments were released and the implants elevated off of the bone. A very thick capsule was found around the implant as expected.
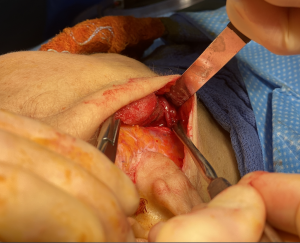

 As the implant were slowly mobilized the facial artery was seen attached to the anterior end of the implant which was along the inferior border. Very careful dissection was done to ensure that the artery was not injured our transected. Once released the implants were delivered out through the SMAS incision. The SMAS was closed and the rest of the facelift then completed.
As the implant were slowly mobilized the facial artery was seen attached to the anterior end of the implant which was along the inferior border. Very careful dissection was done to ensure that the artery was not injured our transected. Once released the implants were delivered out through the SMAS incision. The SMAS was closed and the rest of the facelift then completed.
Case Highlights:
1) Women more so than men may find that a jaw angle implant has a masculinizing effect.
2) Through a facelift a direct approach from the implant’s posterior surface can be done and the recovery improved by avoiding a healed intraoral incision..
3) A facelift approach provides better visualization of the crossing facial artery which should injury occur can be more easily controlled.
Dr. Barry Eppley
Indianapolis, Indiana