

Background: The breasts of a women are far from a static anatomic structure. Over a woman’s lifetime her breasts are exposed to a variety of deforming forces including tissue stretch from pregnancies, weight loss as well as gravity. How much damage the breasts will sustain depends on their initial size as well as the extent of these deforming influences.
As a general rule larger initial breasts will become more severely affected they have the most to lose. With loss of substantial breast volume and the creation of more stretched to skin, the degree of ptosis they will suffer will be significant. With a grade IV ptosis there is a significant need for at least extensive breast lifting. (full breast lift) Volume addition is also likely but the amount of it is a patient-specific decision.
While combining lifts with implants is the most efficient and desired breast restoration surgery, there are good reasons to separate them. It is easy to understand that a full breast lift with a large implant exposes the breast to risks of wound separation and maybe even survival of the nipples. As a result the prudent approach is to do a full breast lift first and then perform the implant augmentation three or four months later. This allows the full extent of each procedure to be maximized if desired. (aka big lift and big implant)
But some breasts are on the edge of whether a staged approach is needed. This is a surgeon’s judgement with the patient understanding that, if done together, there may be a significant need for a secondary revision.
Case Study: This middle-aged female had large D sized breasts when she was younger. Between having children and gravity she developed a large ptotic skin sleeve with little breast volume.
 Under general anesthesia modified full breast lifts was first performed (more limited horizontal scar line) with the simultaneous placement of 650cc moderate plus profile breast implants in the dual plane position.
Under general anesthesia modified full breast lifts was first performed (more limited horizontal scar line) with the simultaneous placement of 650cc moderate plus profile breast implants in the dual plane position.
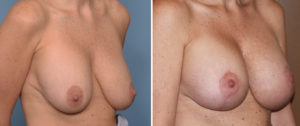
 As can be in her well healed result her breast shape is significantly improved. But some settling of the lift leaves room for a secondary breast lift ‘tuck up’ if desired. This is almost expected as a larger breast implant provides limits as to how much breast skin can be removed during the surgery and the extent of the rest lift achieved. She did it opt for any further breast surgery.
As can be in her well healed result her breast shape is significantly improved. But some settling of the lift leaves room for a secondary breast lift ‘tuck up’ if desired. This is almost expected as a larger breast implant provides limits as to how much breast skin can be removed during the surgery and the extent of the rest lift achieved. She did it opt for any further breast surgery.
Case Highlights:
1) Most sagging and aging breasts have inadequate volume and too much skin.
2) Combining breast lifts with implants must take into consideration how much skin needs to be removed and what implant volume is needed.
3) Full breast lifts with the desire for large implants should be done in separate surgical stages.
Dr. Barry Eppley
Indianapolis, Indiana