


Background: Gendor dysphoria affects many aspects of the face and body in the male to female transitioning patient. For the body wide shoulders is one of the top priorities to change, even surpassing that of breast or buttock augmentation for many transgender patients. Fortunately an operation does exist that directly addresses that concern by shortening the length of the clavicles.
In shoulder narrowing the most common questions about it are: 1) How effective is the procedure?, 2) what are the most significant complication(s) that could occur? and 3) are there any aesthetic tradeoffs for the shoulders becoming less wide? These questions are best answered by looking at a patient’s experience during and immediately after the procedure.
Case Study: This transgender male to female patient had been through previous body contouring procedures including breast implants and multiple liposuction and buttock augmentation procedures. The one finishing body procedure she wanted was a shoulder narrowing procedure. Her current bideltoid distance was 49cms.

 Under general anesthesia a 3 cm bone segment was removed from each clavicle with double plate fixation across the reunited osteotomy sites through a 3.5cm long incision in the supraclavicular fossa. A longer 2.7mm plate is used on the bone’s superior surface and a shorter 2.7mm plate on the anterior surface.
Under general anesthesia a 3 cm bone segment was removed from each clavicle with double plate fixation across the reunited osteotomy sites through a 3.5cm long incision in the supraclavicular fossa. A longer 2.7mm plate is used on the bone’s superior surface and a shorter 2.7mm plate on the anterior surface.
The incision sites are closed in multiple layers with dissolvable subcuticular sutures placed in the skin. Multiple tapes are applied with adhesive over the incision sites. No arm slings or other arm supports are applied afterwards.


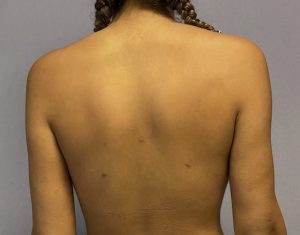
 When seen the next day her shoulder widths were visibly reduced to a 44.5cm bideltoid distance. The change was apparent in both frontal and back views. Every patient initially appears to have a rolled in cholera appearance because of splinting, the more inward shoulder position that provides the most comfort and is part of keeping one’s elbows initially up against one’s side. (mandatory postoperative arm positioning) Bruising and swelling are expected at the incision sites under the tapes but nit swelling occurs at the outer shoulders.
When seen the next day her shoulder widths were visibly reduced to a 44.5cm bideltoid distance. The change was apparent in both frontal and back views. Every patient initially appears to have a rolled in cholera appearance because of splinting, the more inward shoulder position that provides the most comfort and is part of keeping one’s elbows initially up against one’s side. (mandatory postoperative arm positioning) Bruising and swelling are expected at the incision sites under the tapes but nit swelling occurs at the outer shoulders.
 A postoperative x-ray shows good alignment of the clavicles and intact plates and screws.
A postoperative x-ray shows good alignment of the clavicles and intact plates and screws.
 The effectiveness of shoulder narrowing is apparent immediately and is not obscured by any swelling. It has a consistent high satisfaction rating amongst the treated patients. There will be some apparent rolling in of the shoulders that is temporary due to more comfortable shoulder positioning. Pulling the shoulders back initially pulls on the clavicles as well as stretches the upper pectoralis major muscle which has some attachments around the osteotomy sites.
The effectiveness of shoulder narrowing is apparent immediately and is not obscured by any swelling. It has a consistent high satisfaction rating amongst the treated patients. There will be some apparent rolling in of the shoulders that is temporary due to more comfortable shoulder positioning. Pulling the shoulders back initially pulls on the clavicles as well as stretches the upper pectoralis major muscle which has some attachments around the osteotomy sites.
 Besides infection (which has yet to be seen) the only major medical complication is that of fixation failure and bony non-union. The best way to minimize this risk is double plate fixation which resists the displacing forces of arm abduction (superior plate) as well as posterior extension.(anterior plate) The scar outcome and whether the fixation hardware will need to be removed in the future remains to be seen. But whatever their outcome it pales in comparison to avoiding the risk of hardware failure and/or bony non-union of a highly loaded shoulder joint in the early postoperative period.
Besides infection (which has yet to be seen) the only major medical complication is that of fixation failure and bony non-union. The best way to minimize this risk is double plate fixation which resists the displacing forces of arm abduction (superior plate) as well as posterior extension.(anterior plate) The scar outcome and whether the fixation hardware will need to be removed in the future remains to be seen. But whatever their outcome it pales in comparison to avoiding the risk of hardware failure and/or bony non-union of a highly loaded shoulder joint in the early postoperative period.
Case Highlights:
1) Clavicle reduction is an effective procedure for shoulder narrowing that employs a linear length reduction of the bone.
2) While temporary swelling and bruising occurs at the medial incision/osteotomy sites there is no swelling that develops at the outer shoulders.
3) Due to splinting in the immediate postoperative period the shoulders will temporarily look a but rolled in.
Dr. Barry Eppley
Indianapolis, Indiana