

Background: Hip augmentation has turned out to be a more variable procedure than initially perceived. Hip augmentation was largely unknown in plastic surgery prior to BBL surgery. Historically aesthetic hip surgery was about reduction to gain more narrow hips and less full thighs as liposuction was introduced and widely clinically used. Hip augmentation gained traction as the once discarded fat from liposuction was recycled for buttock augmentation and the desire for concomitant lateral hip augmentation to complement it became popular.
Despite a lot of fat injections being done to the hip area a very low percentage of them would be considered successful. As a result silicone hip implants have been used with different designs with variable success. Silicone hip implants are prone to chronic seromas, visible implant edging and implant bending. This is undoubtably related to the use of a subcutaneous pocket for placement as the more favorable subfascial or intra/submuscular pockets are not able to be used in the hip area.
The concept of hip augmentation in the transfemale takes on another conceptual variation. The narrow pelvis width in these patients poses problems for conventional hip implants even if they were highly successful. This patient population often has a skeletal or high hip deficiency that no conventional hip implant can add address. This requires a method for pelvic width increase that provides iliac crest widening or upper hip augmentation. This has now been addressed by an innovative titanium plate design that provides an effective lateral iliac crest augmentation that can be performed with a low rate of complications. But because the plate augments only the skeletal part of the hip it can be predicted that a hip contour deficiency would be created below it particularly if the subiliac indentation or hip dips existed previously. This has created the need for soft tissue hip augmentation below the plate. (subiliac fossa) For a confluent contour between the titanium plate and the silicone implant a need has arisen for a uniquely designed hip implant design that hooks into the titanium plate. This creates a unique two-part hip augmentation system concept.
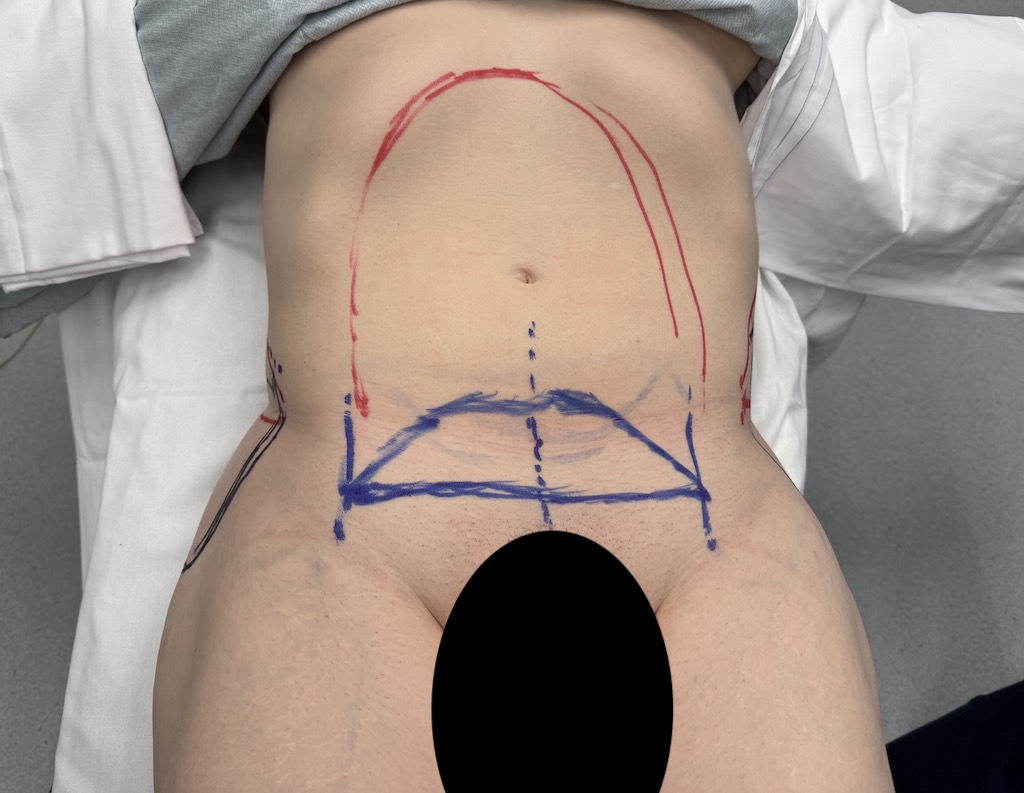
Case Study: This transfemale desired an improved waist to hip ratio/appearance. She had a narrow pelvic width with indented subiliac regions with a broader waist and fuller lower thighs. She also some lower abdominal skin excess and fuller upper inner thighs.
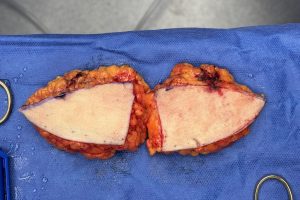 Under general anesthesia abdominal, flank and inner thigh liposuction was performed followed by a mini-tummy tuck to improve the waist.
Under general anesthesia abdominal, flank and inner thigh liposuction was performed followed by a mini-tummy tuck to improve the waist.

 Then 35mm titanium iliac crest plates with three anterior bicortical screws with hooked silicone implants was placed bilaterally.
Then 35mm titanium iliac crest plates with three anterior bicortical screws with hooked silicone implants was placed bilaterally.



 The early clinical results showed the improvement in the waist to hip ratio through widening of the iliac crest and filling in of the subiliac hip dips below it.
The early clinical results showed the improvement in the waist to hip ratio through widening of the iliac crest and filling in of the subiliac hip dips below it.
Skeletal hip augmentation is possible with this innovative titanium plate design for increasing pelvic width. Dissection along the iliac crest is a safe with no significant neurovascular structures located along the way. Because the plate augments only the upper third or skeletal part of the hip it is not unexpected that a hip contour deficiency may be created below it. This would be particularly relevant if the patient has pre-existing hip dips. This has created the need for soft tissue hip augmentation below the plate. While this was done initially with an utrasoft solid round silicone implant it became apparent that it needed to merge with the titanium plate in a more confluent fashion. This has led to the hooked hip implant design which is an extension of the plate as a two-part hip augmentation system if needed. This allows for an implant of 150ccs volume to fit right up against the underside of the iliac crest plate. It is placed through the same incision as the plate. By locking into the plate hip implant stability is assured and inferior edging is largely eliminated because the implant does not have to support its own weight.
Key Points
1) Cheekbone reduction is most effectively done with inward bone positioning using anterior and posterior osteotomies.
2) The anterior zygomatic body osteotomy is performed intraorally and can be done using various bone cut patterns with a reciprocating saw and small plate fixation.
3) The posterior zygomatic arch osteotomy can be done using a preauricular incision with an osteotome without plate fixation.
Dr. Barry Eppley
World-Renowned Plastic Surgeon