


Background: The temples are a unique aesthetic region on the side of the face. It typically has a flat or minimally concave external contour bounded by the bony temporal line superiorly, the lateral orbital rim anteriorly, the zygomatic arch inferiorly and the temporal hairline posteriorly. The temples have a hard tissue base consisting of the union of four skull bones, the frontal, temporal, parietal and sphenoid, which creates a deep concavity known as the temporal fossa. However most of its external contour is created by the volumetric fill of the bony temporal fossa with soft tissue, largely the very thick temporalis muscle and some fat.
With aging the temples can develop a deeper concave appearance (hollowing) which is more likely to occur in females particularly those who are naturally thin. Some of this may be due to loss of muscle tissue but most of it is usually due to fat loss. The suspected culprit is the temporal extension of the buccal fat pad which is well known to sustain volume loss with aging. When temporal hollowing becomes excessive with too deep a concave appearance volumetric enhancement is often sought.
The most common form of temporal augmentation is with injectable synthetic fillers (in an office setting) and fat injections. (in a surgical setting) Each of these treatment approaches has their merits but the sustained volumetric stability is always an issue with their use. Conversely temporal implants offer assured volume in the ranges of 2 to 7ccs based on style and size chosen. Placed in a subfascial pocket on top of the temporalis muscle the historic issues of implant edge visibility as seen in the subcutaneous tissue pocket are completely avoided. The only question for temporal implant placement then is what incisional approach is to be used…with multiple options.

 Case Study: This female had developed deep temporal hollowing and was to undergo multiple facial rejuvenative procedures, one of which was a frontal hairline advancement. She desired a permanent solution to her temporal hollowing and opted for temporal implants. Because her concave temporal contour extended completely though the entire temporal region she needed the extended temporal implant style. The depth of her temporal concavity made the 6mm thick implant a better choice than the 3mm thickness.
Case Study: This female had developed deep temporal hollowing and was to undergo multiple facial rejuvenative procedures, one of which was a frontal hairline advancement. She desired a permanent solution to her temporal hollowing and opted for temporal implants. Because her concave temporal contour extended completely though the entire temporal region she needed the extended temporal implant style. The depth of her temporal concavity made the 6mm thick implant a better choice than the 3mm thickness.
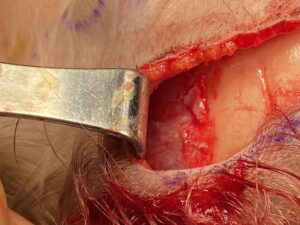

 Under general anesthesia and through her frontal hairline advancement incision the deep temporal fascia was identified at the bony temporal line. The fascia was horizontally incised 5mms below its attachment to leave a cuff of tissue for closure. The subfacial pocket was develop down to the zygomatic arch. The 6mm extended temporal implant was placed and the fascia closed over it. The frontal hairline advancement was then completed.
Under general anesthesia and through her frontal hairline advancement incision the deep temporal fascia was identified at the bony temporal line. The fascia was horizontally incised 5mms below its attachment to leave a cuff of tissue for closure. The subfacial pocket was develop down to the zygomatic arch. The 6mm extended temporal implant was placed and the fascia closed over it. The frontal hairline advancement was then completed.



 The effects of the temporal implant was immediate and made a dramatic correction in her temporal hollows. While the frontal hairline is an uncommon approach to place temporal implants it offers convenient access when it is to be concomitantly performed. It does have the advantage that with the superior access the subfasial pocket developed is able to be kept ‘narrow’ to allow the implant to lie snugly uo against the lateral orbital rim.
The effects of the temporal implant was immediate and made a dramatic correction in her temporal hollows. While the frontal hairline is an uncommon approach to place temporal implants it offers convenient access when it is to be concomitantly performed. It does have the advantage that with the superior access the subfasial pocket developed is able to be kept ‘narrow’ to allow the implant to lie snugly uo against the lateral orbital rim.
Case Highlights:
1) Temporal implants provide a permanent augmentation effect for deep temporal hollowing in females.
2) If a frontal hairline advancement is being performed temporal implants can be placed through this superior approach
3) The implant pocket is created underneath the deep temporal fascia and on top of the muscle with a volumetric effect of up to 7ccs per side.
Dr. Barry Eppley
Indianapolis, Indiana