

Background: Lack of adequate facial projection is a common aesthetic problem that can affects all three levels of the face (facial thirds), often occurring in more than one level in the same patient. The most recognized and treated facial third deficiency is the lower one as commonly seen in a weak chin. It is also the easiest to treat because it involves just a singular point whose projection can be reliably improved by a chin implant or a sliding genioplasty.
Augmentation of the upper and middle third of the face is more challenging due to its larger surface area and more limited incisional access. Midface augmentation is most commonly perceived as that of the cheeks because of the familiarity with standard cheek implants. But true horizontal midface augmentation must consider how to add projection to the maxilla, infraorbital rims and pyriform aperture area. Upper third facial augmentation is more easily understood with increased brow bone and forehead projection but how to do so is not necessarily easy.
The custom facial implant process allows augmentation of any part of the face heretofore not obtainable. While any type of facial implant can be designed, the key questions are the ability to get it positioned in the patient as it is designed and then aligning the implants (if there are multiple ones) once inside the patient to how they are also designed. The custom process allows features to be built into the design to help ensure these important placement issues.
Case Study: This male desired an implant augmentation that brought the entire upper two thirds of the face forward. While he had good chin projection the face above it was more middle recessed. He also desired a more masculine forehead and brow appearance.
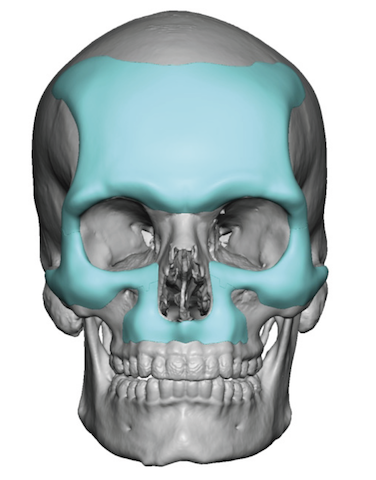
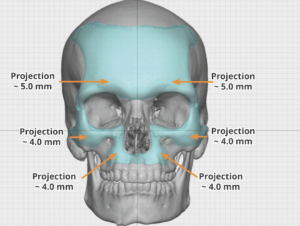 Using his 3D CT scan a custom forehead-brow bone implant was designed to connect to infraorbital implants which then connected to an inferior paranasal-premaxillary implant design. Forward projecting measurements were in the 4 to 5mm range.
Using his 3D CT scan a custom forehead-brow bone implant was designed to connect to infraorbital implants which then connected to an inferior paranasal-premaxillary implant design. Forward projecting measurements were in the 4 to 5mm range.
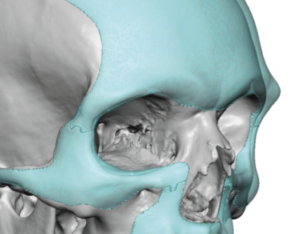 These multiple implants designs were all connected to create a confluent augmentation from the forehead down to the nose. To help with intraoperative placement at the four connections points a geometric type of connection was designed, much like putting a puzzle piece together.
These multiple implants designs were all connected to create a confluent augmentation from the forehead down to the nose. To help with intraoperative placement at the four connections points a geometric type of connection was designed, much like putting a puzzle piece together.
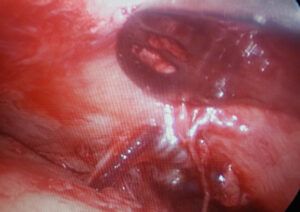
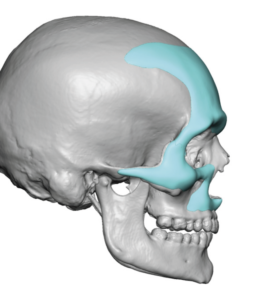
 Under general anesthesia the custom forehead brow bone implant was initially placed using an endoscopic technique. Through the endoscope the tight periosteum along the supraorbital and lateral brow areas was released with preservation of the supraorbital nerves and blood vessels. Bringing the lateral orbital rims component of the custom forehead brow bone implant was aided by the lower eyelid incisions from below.
Under general anesthesia the custom forehead brow bone implant was initially placed using an endoscopic technique. Through the endoscope the tight periosteum along the supraorbital and lateral brow areas was released with preservation of the supraorbital nerves and blood vessels. Bringing the lateral orbital rims component of the custom forehead brow bone implant was aided by the lower eyelid incisions from below.
 Through lower eyelid incisions, the custom infraorbital-malar implants were placed. Because of their large size a vertical geometric split was done through the thickest part of the cheek. This enabled them to be introduced in two smaller pieces and then reassembled once inside. Screw fixation was used on each side of the implant split.
Through lower eyelid incisions, the custom infraorbital-malar implants were placed. Because of their large size a vertical geometric split was done through the thickest part of the cheek. This enabled them to be introduced in two smaller pieces and then reassembled once inside. Screw fixation was used on each side of the implant split.
 The custom premaxillary-paranasal implant was placed intraorally through a high vestibular incision and secured with a single screw for side.
The custom premaxillary-paranasal implant was placed intraorally through a high vestibular incision and secured with a single screw for side.
In this extensive custom forehead-brow bone-infraorbital-malar-premaxillary-paranasal implant, it may be designed as a single piece but can not be placed as such. It must be sectioned and placed through three separate incisional approaches as would be done as if they were separate implants. Ensuring a smooth connection between requires a method that ensures a good fit for which tech geometric split method has proven reliable.
Case Highlights:
1) Extensive building out the face can be done through a series of onlay custom facial implants that are connected like puzzle pieces.
2) The puzzle piece custom implant concept is invaluable when doing extensive implant coverages through limited incisional access.
3) Bring the upper two thirds of the face forward requires augmentation of the entire forehead and brow bones and a line of augmentation along the infraorbital rims and down around the pyriform aperture area.
Dr. Barry Eppley
Indianapolis, Indiana