


Background: Bone fractures of the face are not uncommon due to a variety of external force mechanisms. One of the more common types of facial bone injuries involves the cheekbones, known as the zygomatico-maxillary complex (ZMC) fracture. While typically referred to as a cheekbone fracture its anatomic derangement is more complex than that name implies. With connections to the orbital bone and maxilla, severely depressed/displaced ZMC fractures affect the orbital floor. With significant orbital floor disruption the support of the eyeball is lowered and, as a result, the eyeball will be displaced lower.
Primary repair of the displaced ZMC fractures aims to put the bone back into its original anatomic position and stabilize it with plates and screws. In so doing this may adequately restore the orbital floor. But when it does not the use of an implant or bone graft is done to do so.
But in many severe facial injuries with significant ZMC displacement, even the best primary repair efforts may not create complete anatomic facial restoration. This may be partially due to difficulties in getting complete anatomic bone repositioning, soft tissue atrophy or a combination of both. This may result in a lower position of the eye known as vertical orbital dystopia….technically traumatic vertical orbital dystopia.

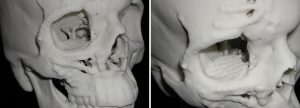 Case Study: This young male had been involved in a severe motor vehicle accident resulting in fractures of the right brow bone and ZMC as well as extensive soft tissue injuries. He had primary bone and soft tissue repairs but, when fully healed, had vertical orbital dystopia of 6mms. Anatomic models made from 3D CT scans showed that the position of the periorbital bones reflected what was seen on the outside….the entire orbital box was lower.
Case Study: This young male had been involved in a severe motor vehicle accident resulting in fractures of the right brow bone and ZMC as well as extensive soft tissue injuries. He had primary bone and soft tissue repairs but, when fully healed, had vertical orbital dystopia of 6mms. Anatomic models made from 3D CT scans showed that the position of the periorbital bones reflected what was seen on the outside….the entire orbital box was lower.
Under general anesthesia the superior orbital rim was elevated with a shaving reduction of the lower bony rim. The orbital floor and rim was bone grafted to the level of 6mms has measured on the anatomic model. A lateral canthoplasty was also performed.
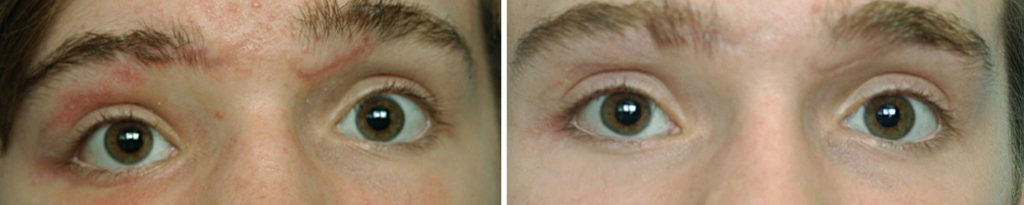 His results demonstrate that substantial improvement of traumatic orbital dystopia is possible because there was an original higher intraorbital space. (the orbital roof is still normal) Raising the perimeter of the orbital box by ostectomies, osteotomies and bone grafting or implants are all methods to do so.
His results demonstrate that substantial improvement of traumatic orbital dystopia is possible because there was an original higher intraorbital space. (the orbital roof is still normal) Raising the perimeter of the orbital box by ostectomies, osteotomies and bone grafting or implants are all methods to do so.
Case Highlights:
1) Traumatic bone injuries to the cheekbone and eye, even after primary surgical repair, can result in a lower position of the eyeball.
2) Secondary reconstruction of the orbital floor through bone graft or implant augmentation and adjustment of the lower eyelid can produce better alignment of the horizontal pupillary level of the eyes.
3) 3D CT scans and anatomic models provide invaluable presurgical planning information.
Dr. Barry Eppley
Indianapolis, Indiana