

Background: The forehead is the largest surface area of the face without distinct features. Between the eyebrows and the frontal hairline lies a surface that, while not completely flat, generally is smooth without obvious prominences. Thus when a bump or projection appears on the forehead it is easily observed. Unless there is hair covering the forehead it is particularly apparent to the patient and often stands out in pictures.
In the male there are normal projections of the lower forehead which are paired brow bones. Projections of the upper forehead, however, are aesthetically unacceptable. Common causes of upper forehead projections include osteomas, forehead horns and generalized asymmetries. In forehead asymmetries the question is always whether its cause is a bony excess or deficiency, which is really determined from the patient’s aesthetic standpoint. More times than not such forehead asymmetries are perceived as bony excesses.
In reduction of forehead asymmetries the critical question is incisional access. Where can the incision be placed that is aesthetically acceptable but still be able to do an adequate bony reduction? The incision must provide adequate reach for high speed burring in particular and/or rasping refinement. It must not be too far behind the upper curve of the forehead as it transitions onto the skull where linear access to the bony protrusion is lost.
Case Study: This male was bothered by a right upper forehead protrusion that transitioned onto the skull behind the hairline. It was particularly noticeable to him in pictures. It was a generalized fullness and not a distinct circular forehead horn.
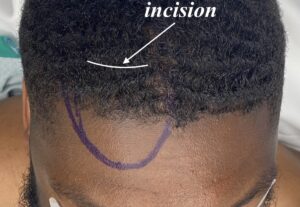
 Under general anesthesia and through a limited scalp placed behind the hairline the bony protrusion was gradually taken down with initial high speed burring. The reduction was completed and smoothed with a series of large toothed diamond rasps.
Under general anesthesia and through a limited scalp placed behind the hairline the bony protrusion was gradually taken down with initial high speed burring. The reduction was completed and smoothed with a series of large toothed diamond rasps.

 The intraoperative change was apparent and care was needed to not avoid over reduction which is easy to do in more modest forehead protrusions. The incision was closed with small dissolvable sutures and a forehead compression was applied for the night after surgery.
The intraoperative change was apparent and care was needed to not avoid over reduction which is easy to do in more modest forehead protrusions. The incision was closed with small dissolvable sutures and a forehead compression was applied for the night after surgery.

 When seen the next day for forehead wrap removal the forehead had an improved symmetry.
When seen the next day for forehead wrap removal the forehead had an improved symmetry.
Most aesthetic bony forehead issues are usually in the upper half of the forehead where hairline or retro hairline incisions provide access for reduction. The key for the incision is that I can not be too far behind the hairline which can obscure linear visual access. While the bone is reduced by a subperiosteal tunnel technique from the incision the vision for the reduction is not unlimited. It takes a combination of internal vision and external palpation to determine just the right amount of bone to remove to improve the bony forehead symmetry.
Case Highlights:
1) Forehead shape concerns are common aesthetic skull deformities because of their visibility in all patients and genders.
2) Bony protrusions of the upper forehead, whether unilateral or bilateral, are particularly noticeable in pictures and various lighting
3) Reducing upper forehead protrusions can be done by various methods from high burring and shaving by rasps.
Dr. Barry Eppley
World-Renowned Plastic Surgeon