


Background: A not uncommon but less frequently treated aesthetic forehead deformity is that of prominent temporal arteries. Seen as ‘squiggly worms’ on the side of the head crossing from the temporal region into the upper lateral forehead they occur for reasons unknown. Their serpiginous pattern and location make them the undeniable course of the anterior branch of the superficial temporal artery.
Why they develop in some people and not others is not known although lack of or loss of subcutaneous fat in the temples helps expose the artery which runs in the connective tissues between the skin and the deep temporal fascia. What is known is that such arterial prominences tend to occur more frequently in men than women. This is likely due to their larger artery sizes and thicker muscular walls, making their course more visible.
But prominent temporal arteries do occur in women and potentially may be more aesthetically bothersome…although their capacity for coverage with various hairstyles makes them easier to hide. When seen in females they often, although not always, have less prominence than in men. But the techniques used to reduce or eliminate them are the same.



 Case Study: This female was bothered by prominent temporal arteries than was most evident on her right side. While the left side was less visible she opted for a bilateral approach since it was unknown if the left side would eventually become more prominent. The arterial pattern and ligation points were marked with three on the right side and two on the left side.
Case Study: This female was bothered by prominent temporal arteries than was most evident on her right side. While the left side was less visible she opted for a bilateral approach since it was unknown if the left side would eventually become more prominent. The arterial pattern and ligation points were marked with three on the right side and two on the left side.


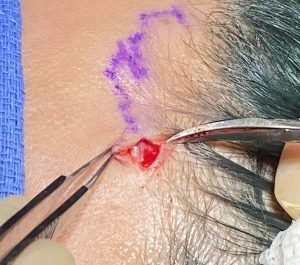
 Under local anesthesia the ligation points were opened up with small incisions, the artery identified and double ligations performed with 5-0 prolene permanent sutures. Because of a persistent doppler signal on the right side a fourth ligation point, lower on the temporal hairline was made to eliminate the signal.
Under local anesthesia the ligation points were opened up with small incisions, the artery identified and double ligations performed with 5-0 prolene permanent sutures. Because of a persistent doppler signal on the right side a fourth ligation point, lower on the temporal hairline was made to eliminate the signal.

 All incisions were closed with 6-0 plain sutures. The tedious nature of the procedure requires an operative time of 6o0 to 90 minutes for both sides.
All incisions were closed with 6-0 plain sutures. The tedious nature of the procedure requires an operative time of 6o0 to 90 minutes for both sides.
While some female temporal arteries may be less prominent than in men, the location and number of ligation points is not less. The key is to use a doppler probe and keep listening for an arterial signal with each ligation site. The number of ligation sites must continue until the doppler signal is eliminated along the course of the artery.
One of the key locations for ligation is every patient that I have treated is out on the lateral mid-forehead near or over the bony temporal line. This is where the arterial takes an abrupt and almost 90m degree turn into the upper forehead heading into the frontal hairline. This is clearly important to cut off the back flow from the scalp. Because it is close to where the frontal branch of the facial nerve runs it is important to isolate the artery before its ligation. While always a potential concern I have never seen a nerve injury. In addition, even though the ligation area is out in the exposed forehead, it has never been a adverse scar issue.
Case Highlights:
1) Prominent temporal arteries occur in women far less frequently than in men and, when they occur, they often are less pronounced.
2) Temporal artery ligation techniques are the same in women as in men and I have not found less ligation points are typically needed.
3) In all temporal ligations the number of ligation points mist progress until its doppler signal is diminished.
Dr. Barry Eppley
Indianapolis, Indiana