

Background: While fat injections and synthetic fillers are the most common methods of cheek augmentation, implants still have a useful role to play. But when cheek implants have been placed previously and the patient desires additional volumetric enhancement later, the question becomes what is the best method to do so. The answer to that question is multi-factorial… how long ago were the cheek implants done, are there any problems with the existing cheek implants, does one want a temporary vs permanent additive change, are other facial surgery procedures being planned and what is the age of the patient? In short the answer will vary based on each patient’s situation and desired.
The obvious and simple answer is just do injectable fillers or even fat injections on top of the cheek implants. There is always an adequate subcutaneous tissue layer in which they can be placed. But if the existing cheek implants have issues and the patient does not want to pursue an injectable approach then cheek implant replacement may be the best approach.
When considering cheek implant replacements it is almost always true that a custom design approach offers the most predictable change. The existing cheek implants provide a blueprint from which to make the desired changes as they have a known outcome. A 3D CT scan allows the cheek implants to be seen…provided they are of a material which can be seen radiographically. But what if they can’t be visualized…..
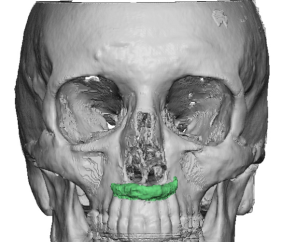
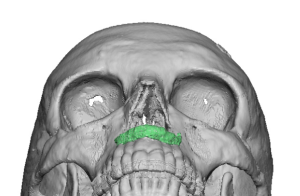 Case Study: This older female had a history of cheek implants placed over 20 years ago. She had a lot of initial problems on the left side which numbness and facial nerve weakness. While most of these early postoperative symptoms eventually improved she always had a feeling of cheek tightness on that side. Now that she was older and had developed loose sagging cheek tissue over the implants she desired larger cheek implant replacements for a combined size increase and to achieve a ‘cheek lift’ from them. Her 3D CT scan did not show any cheek implants which confirmed they were of a porous polyethylene (Medpor) material. A premaxillary implant was present, most likely of an ePTFE (Goretex) rolled material placed at the time of her rhinoplasty. There was a distinct imprint across the face of the maxilla and across the cheekbone which indicated there was an implant there of Medpor material but of unknown projection.
Case Study: This older female had a history of cheek implants placed over 20 years ago. She had a lot of initial problems on the left side which numbness and facial nerve weakness. While most of these early postoperative symptoms eventually improved she always had a feeling of cheek tightness on that side. Now that she was older and had developed loose sagging cheek tissue over the implants she desired larger cheek implant replacements for a combined size increase and to achieve a ‘cheek lift’ from them. Her 3D CT scan did not show any cheek implants which confirmed they were of a porous polyethylene (Medpor) material. A premaxillary implant was present, most likely of an ePTFE (Goretex) rolled material placed at the time of her rhinoplasty. There was a distinct imprint across the face of the maxilla and across the cheekbone which indicated there was an implant there of Medpor material but of unknown projection.
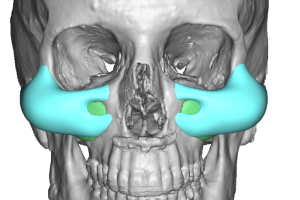
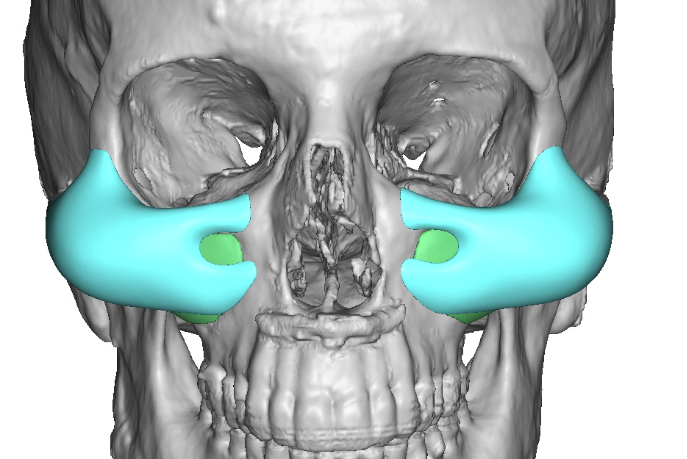
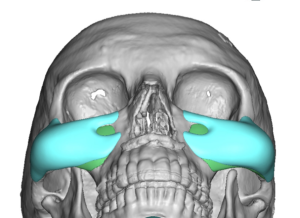 In designing cheek implant replacements it had to be presumed that the existing implant footprints were too low on the maxilla and their thicknesses were probably no more than m3 or 4mm maximum. Thus new cheek implants were designed adding in the estimated existing cheek implant thicknesses for a total projection of 12mms.
In designing cheek implant replacements it had to be presumed that the existing implant footprints were too low on the maxilla and their thicknesses were probably no more than m3 or 4mm maximum. Thus new cheek implants were designed adding in the estimated existing cheek implant thicknesses for a total projection of 12mms.
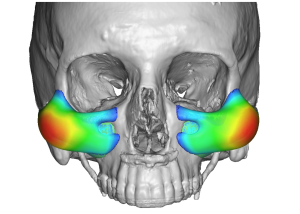 One key element in any cheek implant design is where is the location and shape of the maximum projection. As a female and compatible with her goals it was located over the typical female cheekbone area but in a higher position so as to also have a significant lifting effect.
One key element in any cheek implant design is where is the location and shape of the maximum projection. As a female and compatible with her goals it was located over the typical female cheekbone area but in a higher position so as to also have a significant lifting effect.
 Under general anesthesia and through an intraoral approach the implants were quickly discovered right under the mucosal incision and were Medpor material. The Medpor cheek implants, which were tenaciously attached to the overlying soft tissues, were removed. (challenging to do but always can be successfully done) Due to the dissection needed for the implant removals an adequate pocket existed for the new custom cheek implants. The shape and size differences between the new vs old cheek implants could be seen by a side by side comparison.
Under general anesthesia and through an intraoral approach the implants were quickly discovered right under the mucosal incision and were Medpor material. The Medpor cheek implants, which were tenaciously attached to the overlying soft tissues, were removed. (challenging to do but always can be successfully done) Due to the dissection needed for the implant removals an adequate pocket existed for the new custom cheek implants. The shape and size differences between the new vs old cheek implants could be seen by a side by side comparison.

 Placing the new custom cheek implants on the patient showed what a significant change in cheek projection that would be achieved.
Placing the new custom cheek implants on the patient showed what a significant change in cheek projection that would be achieved.

 The new cheek implants were placed high up on the cheekbones and secured with a screw, well away from the mucosal incision and the bony face of the maxilla.
The new cheek implants were placed high up on the cheekbones and secured with a screw, well away from the mucosal incision and the bony face of the maxilla.
Despite the frequent comments that I hear that Medpor facial implants are impossible to remove I have done it successfully hundreds of times. I didn’t say it was easy as the soft tissue attachments are significantly ingrown but there are intraoperative techniques that make it possible. As always with Medpor implant removals it is going to be traumatic to the surrounding soft tissues so the potential for adjacent nerve injuries are always possible and the postoperative tissue swelling may be significant. If implant replacements are being done at the same time the one ‘advantage’ of removing Medpor implants is that the pocket for the new implants is usually largely made due to the amount of soft tissue dissection needed.
Case Highlights:
1) Medpor cheek implants are often not seen on 3D CT scans…which can make their implant replacement planning less than precise.
2) Extensive dissection and soft tissue releases are necessary for Medpor cheek implant removals which does place the infraorbital and terminal branches of the buccal nerves at risk for injury.
3) Custom cheek implant replacement designing must take into consideration the existing footprint and projection of the indwelling cheek implants.
Dr. Barry Eppley
Indianapolis, Indiana