


Background: Many different body muscle groups can be successfully augmented with aesthetic implants. The most common, both by history and clinical use, are for the pectoral, buttock and calf muscles. From pectoral implants has sprung the need for other upper body implants to complement them for the arms and shoulders. (bicep, tricep, and deltoid muscles)
Deltoid implants are unique amongst body implants due to the anatomy of the deltoid muscle. The deltoid muscle is responsible for the rounded contour of the shoulders. It has its origin from the end of the clavicle and the spine of the scapula, going it a broad superior surface area. The broad three heads of the muscle converge inferiorly to insert onto the mid-shaft area of the humeral bone. This anatomy poses some challenges for implant augmentation as there is no natural gliding movement of the muscle. The muscle is tight and very adherent around the shoulder since one of its primary functions is to prevent dislocation of the humeral head during load bearing. (which also protects the axillary nerve)
Deltoid implant locations could be on top of the muscle (subfascial), intramuscular or submuscular. The subfascial location offers the easiest dissection and the highest implant location if done from a superior skin incision next to the AC joint. But the risk of implant show is fairly high being in a more superficial location. The submuscular location avoids the risk of implant show but getting under the tight deltoid muscle is difficult and the natural tendency is for the implant to migrate inferiorly due to the very tight upper portion of the muscle as it wraps around the shoulder. In some cases surgeons may opt for placing inside the muscle which is no easier than placing it submuscular.
There is no consensus as to the best method for deltoid implant placement. Although the few surgeons that perform it usually opt for submuscular placement using either an anterior or posterior axillary approach. But the risk of implant displacement/malposition is not insignificant. Managing undesired deltoid implant results pose challenges.


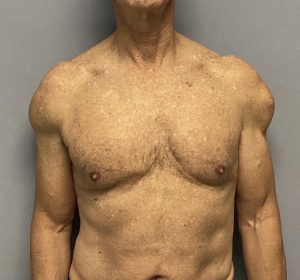
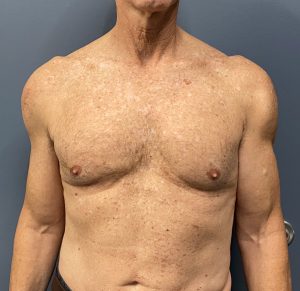
 Case Study: This older male presented with having four prior deltoid implant surgeries as well as fat grafting to the shoulders. He had low implant placements on both sides with a sharp edge of the implant visible on the left side. There were vertical scars over the mid-deltoid areas. He also had pectoral and bicep implants as well of which he had no concerns.
Case Study: This older male presented with having four prior deltoid implant surgeries as well as fat grafting to the shoulders. He had low implant placements on both sides with a sharp edge of the implant visible on the left side. There were vertical scars over the mid-deltoid areas. He also had pectoral and bicep implants as well of which he had no concerns.
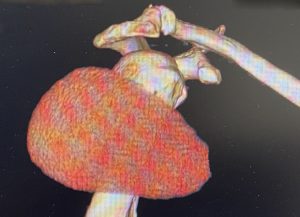
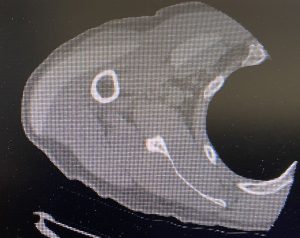 To fully understand the shape, size and position of his deltoid implants a 3D CT scan was obtained. The right deltoid implant showed a calf implant placed longitudinally most of which was under some muscle.
To fully understand the shape, size and position of his deltoid implants a 3D CT scan was obtained. The right deltoid implant showed a calf implant placed longitudinally most of which was under some muscle.


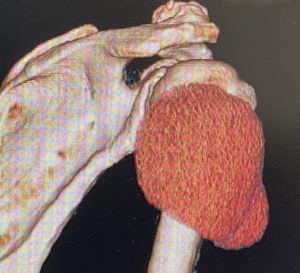
 The left deltoid implant showed what looked like the same implant as the other side but its anterior end appeared cut off. The front edge of the implant was clearly outside the muscle.
The left deltoid implant showed what looked like the same implant as the other side but its anterior end appeared cut off. The front edge of the implant was clearly outside the muscle.
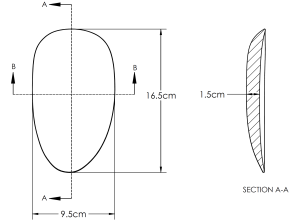 Custom deltoid implants were designed using the existing right side implant’s shape (foot print) and extending it upper superiorly to fill in what was missing at the top of the shoulder. It also had some additional length of 1 cm as well as much more feathered edges. The new implants had a volume of 127ccs.
Custom deltoid implants were designed using the existing right side implant’s shape (foot print) and extending it upper superiorly to fill in what was missing at the top of the shoulder. It also had some additional length of 1 cm as well as much more feathered edges. The new implants had a volume of 127ccs.


 Under general anesthesia the vertical shoulder incisions were used for access and the existing deltoid implants removed. What was initially thought to be an implant that had been cut off before surgery turned out to be a ‘fractured ‘ implant where the front end of the implant was found behind the larger implant piece. Comparing the removed vs the new implants showed the difference between them both out on a table as well as overlaid on his shoulders.
Under general anesthesia the vertical shoulder incisions were used for access and the existing deltoid implants removed. What was initially thought to be an implant that had been cut off before surgery turned out to be a ‘fractured ‘ implant where the front end of the implant was found behind the larger implant piece. Comparing the removed vs the new implants showed the difference between them both out on a table as well as overlaid on his shoulders.
Most body implants once they are implanted are very difficult to adjust their encapsulated pockets later. Only breast implants offer relative ease in adjusting their pockets as they are round with almost equal access to all parts of them and with two favorable incision locations. (inframammary and periareolar) This when deltoid implants are low positioned the ability to raise the pocket is both very difficult and highly unsuccessful. A more effective strategy is to design an implant that uses the existing inferior capsule location and creates the superior fill needed with a higher implant design.The upper part of the pocket can be expanded but it is near to impossible to raise up a pocket that is too low and have it stay high. In other words a more effective solution is to DESIGN AN IMPLANT THAT CAN WORK WITH THE EXISTING POCKET RATHER THEN TRYING TO MAKE THE POCKET FIT AN EXISTING IMPLANT.

 His one month postoperative result showed the improved shoulder shape with a more natural appearance.
His one month postoperative result showed the improved shoulder shape with a more natural appearance.
One interesting observation in this case is why did the left deltoid implant fracture? I would presume the surgeon didn’t deliberately tear the implant or cut it that way. What undoubtably happened is the pocket was smaller than the implant (which the surgeon didn’t fully realize and when the implant was inserted it need ended up folded on itself…unknown to the surgeon as that can not be seen through such a small incision. The folded implant eventually torn along the fold inadvertently creating a double stacked implant with a sharp edge.
Case Highlights:
1) The most common deltoid implant malposition is an inferior displacement or too low on the muscle.
2) The best way to fully understand the actual shape and position of an existing malpositoned deltoid implant is a 3D CT scan.
3) Given the difficulty of raising up an inferiorly displaced deltoid implant pocket it is usually best to design an implant that maintains the inferior extent of the pocket and provides a more superior augmentation that is closer to the level of the AC joint.
Dr. Barry Eppley
World Renowned Plastic Surgeon