

Background: Fractures of the lower jaw are one of the most common types of facial fractures. While in adults such fractures may often occur from fights, in younger patients sporting events and recreational activities are the more common sources. Also in younger patients the severity of the mandibular fracture in terms of bone displacement is often less due to the greater plasticity of growing bones. As a result non- or minimally displaced mandible fractures are more common in these younger patients.
Displaced mandible fractures are almost always treated by open reduction and internal fixation using metal plates and screws. In non-displacements or very minimal displacements a closed reduction using intermaxillary fixation of the teeth can be an effective treatment. When using metal plates and screws for such fracture fixation, many such devices do not need to be removed in adults unless they are in close proximity to the teeth or mental nerve or become loose over time. In children where ongoing bone growth is to be expected and permanent teeth eruption may not have fully occurred, such metal hardware may need to be subsequently removed.
One bone fixation technique that would avoid the potential need for removal later is the use of non-metal or resorbable plates and and screws. Such resorbable fixation materials have been available for clinical use for over twenty years. While primarily developed for pediatric cranial vault surgery, they have been used in other applications from orthognathic surgery to adult midface/orbital/skull fractures.
Case Study: This 9 year-old male fell from a bicycle sustaining bilateral mandible fractures. The fractures were in the classic parasymphyseal (left) and contralateral jaw angle (right) locations. Both fracture locations had displacement.
 Under general anesthesia the occlusion was initially put together used twisted arch wires at canines put together in a cross arch fashion.
Under general anesthesia the occlusion was initially put together used twisted arch wires at canines put together in a cross arch fashion.

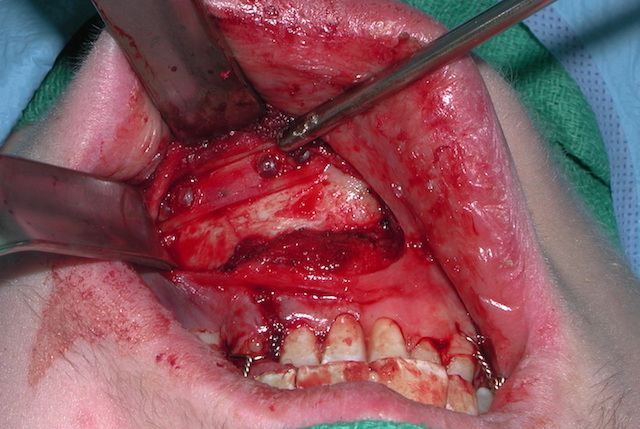
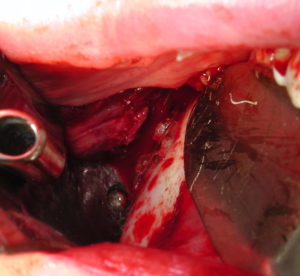 Then through intraoral incisional approaches initially the left parasymphyseal fracture was aligned and secured with a 4 hole resorbable plate and screws. Then the right jaw angle fracture was aligned and stabilized with a 6 hole reservable plate and screws done through a trocar method for screw tapping and insertion.
Then through intraoral incisional approaches initially the left parasymphyseal fracture was aligned and secured with a 4 hole resorbable plate and screws. Then the right jaw angle fracture was aligned and stabilized with a 6 hole reservable plate and screws done through a trocar method for screw tapping and insertion.
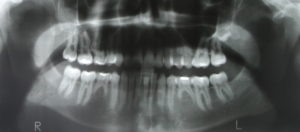

 At the end of the surgery the cross arch wires were removed. A one week after surgery x-ray (panorex) showed good alignment of the fracture sites. He went on to heal successfully with no long term jaw motion or occlusal abnormalities.
At the end of the surgery the cross arch wires were removed. A one week after surgery x-ray (panorex) showed good alignment of the fracture sites. He went on to heal successfully with no long term jaw motion or occlusal abnormalities.
While reservable plate and screw fixation has tremendous appeal, it is important to recognize that it provides less structural rigidity to fractures sites than does metal fixation devices. Thus its use needs to be reserved for those facial bone applications where stability requirements are less. Pediatric facial fractures is one such application where the bones heal quicker and and the bone support needed is less and for a shorter period of time.
Case Highlights:
1) Displaced mandible fractures in children and early teens can be successfully treated by resorbable plate and screw fixation
2) To help establish intraoperative occlusion for mandible fracture repair in young patients, simple cross arch wires can be used.
3) Due to the rapid healing of young bones, postoperative immobilization is either not needed or only needs to remain in place for ten days.
Dr. Barry Eppley
Indianapolis, Indiana