


Background: Rib pain can develop from a variety of causes, many of which have a specific traumatic or incident history. Short of a rib fracture or underlying pathology in which the rib pain is a symptom, there are a variety of different causes of rib pain that typically have a specific event origin. While they all share the common symptom of pain, they have been given a variety of names which can be diagnostically confusing.
Non-fracture rib pain conditions that can respond to surgery can generally be divided into two main types, the so called slipped rib and the rib tip syndrome. Both share two man symptoms, site-specific pain and clicking. The slipped rib syndrome is when the cartilage on the lower rib slips or moves leading to pain. it goes by a lot of names such as clicking rib and displayed rib to name a few. In this rib condition a mobility of the rib usually refers to ribs #8, 9 or 10 and their cartilaginous junction with the bone. The bony rib becomes disarticulated from its more anterior cartilaginous portion (costochondral junction separation) Mobility at the bone-cartilage junction either impinges on the intercostal nerve or causes inflammation due to periosteal/perichondrial irritation. The clicking is the two ends moving against each other.
Inferiorly lies the free floating or unattached ribs #11 and 12 from which the iliac-costal or rib tip syndrome can occur. This is when the ends or cartilaginous tips of these ribs, which angulate down much more inferiorly than commonly perceived, touch the iliac crest causing pain. This usually occurs when turning from side to side or bending over. The clicking here is the end of the rib rubbing against the crestal bone.
Case Study: This male had a history of working out on a rowing machine pulling heavy weights when he heard a pop on his right side with immediate pain. Over the course of the following year he had extensive workups to rule out spinal nerve impingement as the source of his pain which were all negative. Physical therapy and epidural injections failed to provide any improvement. His one consistent physical finding was that of a very specific area of point tenderness that was localized over the lateral chest wall area of ribs #10 and #11. Due to his thick torso tissue layers it was not possible to precisely determine the specific rib. He presented with the diagnosis of ‘slipped rib’.
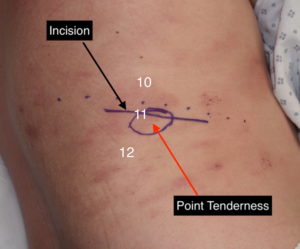
 Under general anesthesia and in the left lateral decubitus position an incision was made with the area of point tenderness at its mid-portion. Dissection was carried to down to the underlying rib which was identified as rib #11 due to angulation and mobility. At the level of the lateral border of the erector spinae muscle, a cut was made through the bony rib. The bony rib was then circumferentially dissected out down to its cartilaginous tip where it was removed. The associated intercostal neurovascular bundle was double ligated with hemaclips at the proximal bony cut. The cavity left behind by the rib removal was filled with Exparel-soaked gelfoam sponges and the periosteum and muscle layer closed over it. An additional 80ccs of Exparel solution was injected into the latissimus dorsi muscle as well as the subcutaneous tissues around the incision site. Exploration was also done on rib #10 which showed an intact bony portion and stable costochondral junction. No rib mobility was detected.
Under general anesthesia and in the left lateral decubitus position an incision was made with the area of point tenderness at its mid-portion. Dissection was carried to down to the underlying rib which was identified as rib #11 due to angulation and mobility. At the level of the lateral border of the erector spinae muscle, a cut was made through the bony rib. The bony rib was then circumferentially dissected out down to its cartilaginous tip where it was removed. The associated intercostal neurovascular bundle was double ligated with hemaclips at the proximal bony cut. The cavity left behind by the rib removal was filled with Exparel-soaked gelfoam sponges and the periosteum and muscle layer closed over it. An additional 80ccs of Exparel solution was injected into the latissimus dorsi muscle as well as the subcutaneous tissues around the incision site. Exploration was also done on rib #10 which showed an intact bony portion and stable costochondral junction. No rib mobility was detected.
This case is unusual in that the area of tenderness was very specifically localized not at the costochondral junction of rib #10 or at the end of rib #11…but at the midportion of bony rib #11. This is not a typical presentation for any of the rib pain syndromes but yet responded to rib resection along the site of point tenderness.
Case Highlights:
1) The most common non-fracture rib pain conditions are the slipped rib and rib tip syndromes which have specific areas of symptom location. They defy diagnostic testing, clinical examination and history are more important and are often a diagnosis of exclusion.
2) Rib removal with or without intercostal nerve resection is the definitive treatment should time and non-surgical therapies not provide symptom improvement.
3) Reproducible point tenderness along a specific rib area is the key in determining whether surgery may be effective.
Dr. Barry Eppley
Indianapolis, Indiana