

Background: The width/shape of the waistline is influenced by numerous anatomic factors, much of which is soft tissue related. The amount of overlying skin, thickness of the subcutaneous fat layer, lateral projection of the latissimus dorsi muscle and even the intra-abdominal space/contents all influence the girth of the waistline. The one hard tissue contribution to it is that of the ribs, specifically the lower ribcage.
The lower ribcage consists of a combination of the false and floating ribs. Ribs #11 and 12 are the free floating ribs (without any attachments) and rib #10 is classified as a false rib because it does not articulate directly with the sternum. (but it has an anterior attachment to rib #9) All three of these lower ribs do have an influence on the width of the waistline as they provide structural support for surrounding soft tissues such as muscles and fascia. Thus a reduction in their lengths will result in some soft tissue collapse inward, reducing the profile of the waistline.
An interesting question is which of the lower ribs makes the biggest contribution to waist reduction? While it clearly is an effect of all three ribs, ribs#10 and #11 make the biggest contribution based on the lengths that are capable of being removed in my observations. Rib #12 is the shortest of the lower three and the shortest of the entire ribcage. It has no costal groove (for the intercostal nerve) and its short tip has a cartilaginous end. It is also prone to underdevelopment or no development at all.

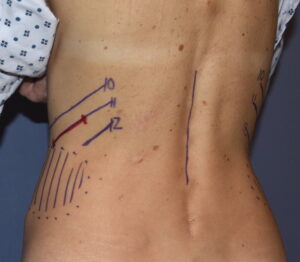 Case Study: This thin female desired to a more shapely waistline even though she was already thin and small framed. Her lower ribcage was almost visible through her skin. Ribs #10, 11 and 12 on the left side were easily palpable and marked. On the right side rib #12 was hard to find but no significance was given to it.
Case Study: This thin female desired to a more shapely waistline even though she was already thin and small framed. Her lower ribcage was almost visible through her skin. Ribs #10, 11 and 12 on the left side were easily palpable and marked. On the right side rib #12 was hard to find but no significance was given to it.

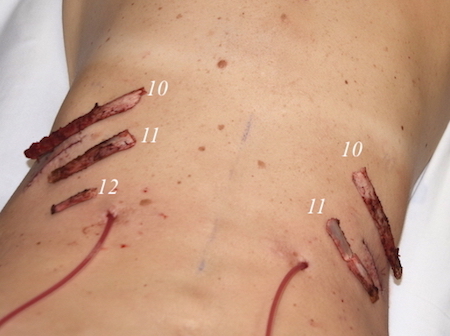
 Under general anesthesia in the prone position flank liposuction was initially performed with only small volumes obtained as expected. Centered over rib #11 a 4.5cm oblique skin incision was made. With the LD muscle split ribs #10 and 11 were exposed preserving the intercostal neuromuscular bundle.
Under general anesthesia in the prone position flank liposuction was initially performed with only small volumes obtained as expected. Centered over rib #11 a 4.5cm oblique skin incision was made. With the LD muscle split ribs #10 and 11 were exposed preserving the intercostal neuromuscular bundle.

 Subtotal rib removals were then done on #10, 11 and 12 using a tunnel technique. Once the ribs were removed the periosteal sleeve was closed over gel foam soaked in Exparel local anesthetic. A strip of latissimus dorsi muscle was removed from the lateral border to supplement the waist narrowing effect.
Subtotal rib removals were then done on #10, 11 and 12 using a tunnel technique. Once the ribs were removed the periosteal sleeve was closed over gel foam soaked in Exparel local anesthetic. A strip of latissimus dorsi muscle was removed from the lateral border to supplement the waist narrowing effect.

 The interesting finding in the case was that rib #12 in the right side could not be found despite extensive exploration…leading to the conclusion that it was congenitally absent.
The interesting finding in the case was that rib #12 in the right side could not be found despite extensive exploration…leading to the conclusion that it was congenitally absent.
 Congenital absence of rib #12 on one side is not unheard of. Because it is the smallest rib it may be prone to a higher incidence of hypoplasia or complete absence.
Congenital absence of rib #12 on one side is not unheard of. Because it is the smallest rib it may be prone to a higher incidence of hypoplasia or complete absence.
Case Highlights:
1) The thin female with an already small waistline is a not infrequent request for rib removal surgery.
2) The goal of the thin female is to have less of a straight line or boyish body shape.
3) The 12th rib is the smallest of all the ribs and can be very short and in rare cases even missing.
Dr. Barry Eppley
Indianapolis, Indiana