

Background: Lower facial or jaw asymmetry is one of the most common forms of facial asymmetry. The projecting nature of the chin/lower jaw, its paired development from the embryonic brachial arches and the relative complexity of the mandibular shape with its various attached soft tissues creates a lot of potential for an asymmetric shape. While jaw asymmetry can occur in pure isolation, it is far more common to be part of an overall facial asymmetry.
When treating jaw asymmetry the historic approach is to make a treatment plan based on its external appearance. Plain x-rays such as a panorex were used to supplement the external appearance evaluation. But the approach was largely an eyeball assessment of what was felt ti be deficient. Procedures such as a centering sliding genioplasty and jaw angle implants were common. That may or may not have been supplemented with soft tissue fat injections either during the primary procedure or done secondarily.
The contemporary approach to jaw asymmetry assessment and treatment planning is through the use of a 3D CT scan. Its value is that it provides a more complete understanding of the scope of the bony asymmetry. Almost all jaws asymmetries in my experience involve the entire jawline and not just the corners. (chin and jaw angle) This makes senses from a developmental standpoint which subsequently makes treatment planning more accurate.
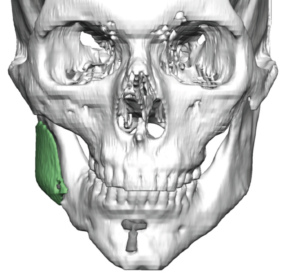
 Case Study: This male a congenital right facial asymmetry. To treat his most prominent right jaw asymmetry he previously had a sliding genioplasty which shifted his chin to the left as well as a standard widening jaw angle implant placed. By augmenting/shifting the two corners, the jawline is stretched out and hence made more symmetric.
Case Study: This male a congenital right facial asymmetry. To treat his most prominent right jaw asymmetry he previously had a sliding genioplasty which shifted his chin to the left as well as a standard widening jaw angle implant placed. By augmenting/shifting the two corners, the jawline is stretched out and hence made more symmetric.
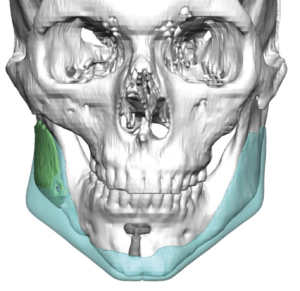
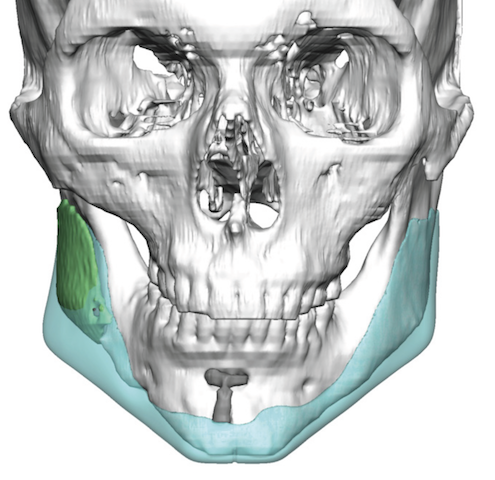
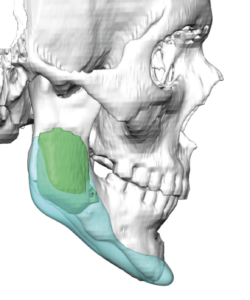
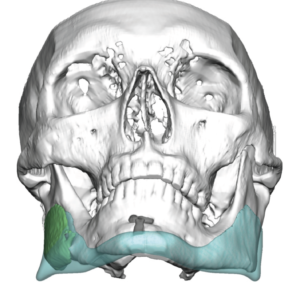 In addition to providing further improvement of his jaw asymmetry he also wanted to take advantage of the opportunity for overall jawline enhancement as well. Using his 3D CT scan a custom jawline implant was designed for those effects and its aesthetic improvement the prior surgery could be when the implanted design was overlaid on the previous sliding genioplasty and jaw angle implant.
In addition to providing further improvement of his jaw asymmetry he also wanted to take advantage of the opportunity for overall jawline enhancement as well. Using his 3D CT scan a custom jawline implant was designed for those effects and its aesthetic improvement the prior surgery could be when the implanted design was overlaid on the previous sliding genioplasty and jaw angle implant.
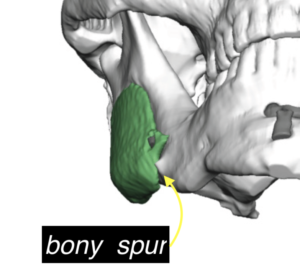
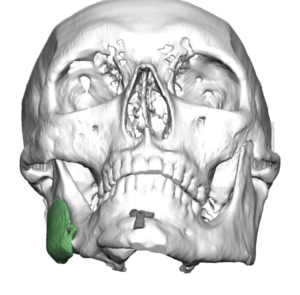
 Under general anesthesia and with the usual three incisional approach for a total jawline implant, the plate from the sliding genioplasty could be seen and the removal of the jaw angle implant done. After removal of the jaw angle implant a bony outgrowth (spur) needed to be reduced and posterior and inferior capsulectomies done to accommodate the new implant.
Under general anesthesia and with the usual three incisional approach for a total jawline implant, the plate from the sliding genioplasty could be seen and the removal of the jaw angle implant done. After removal of the jaw angle implant a bony outgrowth (spur) needed to be reduced and posterior and inferior capsulectomies done to accommodate the new implant.

 The jawline implant was inserted by a midline split technique due to the thickness/stiffness of the right jaw angle material. I did not feel that the implant could be passed anteriorly under the mental nerve in a one piece anterior approach without risk of injury. It was reunited in the midline and double screwed in place as was the jaw angle areas.
The jawline implant was inserted by a midline split technique due to the thickness/stiffness of the right jaw angle material. I did not feel that the implant could be passed anteriorly under the mental nerve in a one piece anterior approach without risk of injury. It was reunited in the midline and double screwed in place as was the jaw angle areas.
The use of a custom jawline implant design allows for both the best asymmetry correction as well as an overall jawline augmentation effect.
Highlights:
- Eyeballing jaw asymmetry correction may offer some improvement but almost always results in an incomplete correction.
- Jaw asymmetry is best treatment planned using the aid of a 3D CT scan.
- A custom jawline implant offers the most complete and effective treatment for many jaw asymmetries.
Dr. Barry Eppley
Indianapolis, Indiana