

Background: The labiomental fold or sulcus only becomes aesthetically relevant when it is seen as too deep. Or what may happen to it when a chin augmentation procedure is considered. How to manage an undesirably deep labiomental fold is most commonly treated by injectable fillers or fat…which works well in most cases in the unoperated chin which is unscarred.
But in the scarred chin trying to bring out a deep labiomental fold by volumetric injections does not usually work well. This is particularly relevant after a sliding genioplasty when the collapse of the soft tissues beneath the fold into the step bony defect can potentially be a source of labiomental dermal adhesion and tightness.
Treating the contracted labiomental fold is typically seen externally as a v-shaped fold. Trying to pull out the labiomental fold adhesion demonstrates tightness and limited lip stretch. When this type of deep labiomental fold is present only an intraoral release will reliably work and to prevent its recurrence an interpositional fat graft is needed. I have found this technique to be consistently effective with either complete or partial resolution of the labiomental symptoms and appearance.
 Case Study: This male had a prior sliding genioplasty as part of orthognathic surgery that resulted in a very deep labiomental fold contracture with lower lip tightness and incompetence. An intraoral release with a dermal fat graft was initially performed 4 months previously. This eliminated his lower lip incompetence and some of the tightness but the depth of the fold was still bothersome to him.
Case Study: This male had a prior sliding genioplasty as part of orthognathic surgery that resulted in a very deep labiomental fold contracture with lower lip tightness and incompetence. An intraoral release with a dermal fat graft was initially performed 4 months previously. This eliminated his lower lip incompetence and some of the tightness but the depth of the fold was still bothersome to him.

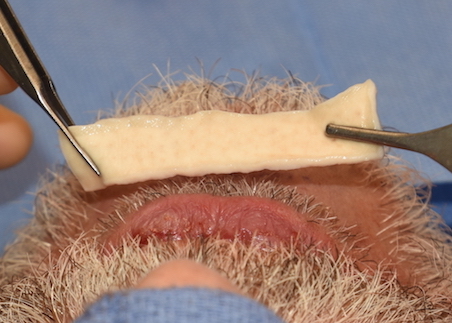
 Under local anesthesia the previous intraoral mucosal incisonal scar was reopened and the previously placed dermal-fat graft identified….at least 50% of which appeared to have survived. The skin of the overlying labiomental fold was released and a pocket developed between the fat graft and the overlying skin. A thick Alloderm graft was hydrated and cut into a 1 x 4 mms long graft.
Under local anesthesia the previous intraoral mucosal incisonal scar was reopened and the previously placed dermal-fat graft identified….at least 50% of which appeared to have survived. The skin of the overlying labiomental fold was released and a pocket developed between the fat graft and the overlying skin. A thick Alloderm graft was hydrated and cut into a 1 x 4 mms long graft.

 The Alloderm graft was threaded into the pocket using a percutaneous suture technique on each side. This ensured that the graft was adequately stretched out and laid flat in the pocket. The remainder of the graft was placed beneath the first graft. The mucosal incision was then closed over it.
The Alloderm graft was threaded into the pocket using a percutaneous suture technique on each side. This ensured that the graft was adequately stretched out and laid flat in the pocket. The remainder of the graft was placed beneath the first graft. The mucosal incision was then closed over it.
The Alloderm grafts used the previously placed dermal-fat graft as a platform for support to help push out on the deepest part of the fold. In a relatively non-mobile area like the labiomental fold I could expect the Alloderm graft to have good persistence.
The deeply contracted labiomental fold requires intraoral release and interpositional graft between it and the bone for noticeable and persistent improvement. Its success depends on how well the dermal fat graft persists…of which some always does. If suboptimal improvement is obtained a second stage graft can be done of which changing to a more rigid graft material likely improves the chance of even further improvement in the depth of the fold.
Case Highlights:
1) The deep and contracted labiomental fold requires release and an interpositonal graft for improvement.
2) A first stage dermal-fat graft is usually sufficient for the interpositional graft because of the volume it provides.
3) When a second stage interpositional graft is needed an allogeneic or tissue back dermal graft can suffice.
Dr. Barry Eppley
Indianapolis, Indiana