

Background: Lip reconstruction from congenital deformities (cleft lip), trauma and cancer resections uses a variety of long standing plastic surgery techniques. When the upper lip tissues are grossly deficient or highly scarred, an historic and valuable reconstruction method is that of the cross-lip flap. (Abbe flap) By transferring unscarred normal vermilion and skin from the usual thicker lower lip, it is inset into the upper lip after discarding the deficient central section.
While the cross lip flap brings fresh tissue into the upper lip, it should never be viewed as the final result. Keeping it alive during the critical first few weeks when the flap is still connected to the lower lip is what is initially important. Once the flap is released from the lower lip and has healed, it can be manipulated into a better shape 6 months (or years) later.
Secondary efforts (revisions) to reshape the upper lip incorporates a variety of techniques, some of which are best known in lip reconstruction while others are more commonly used in aesthetic lip surgery. The plastic surgeon must use every available technique, often done at the same time, to try and get the best upper lip shape.
 Case Study: This female had a poor history of upper lip trauma which was initially reconstructed with a cross lip flap in another country. While good lip tissue existed it did not yet have the best lip shape. Her goals were to have 1) a shorter upper lip length, 2) a unified prolabial aesthetic unit, 3) more narrow philtral scars, 4) a better cupid’s bow shape, 5) a smoother upper lip smile line and 6) release of scar constractures at the mouth corners.
Case Study: This female had a poor history of upper lip trauma which was initially reconstructed with a cross lip flap in another country. While good lip tissue existed it did not yet have the best lip shape. Her goals were to have 1) a shorter upper lip length, 2) a unified prolabial aesthetic unit, 3) more narrow philtral scars, 4) a better cupid’s bow shape, 5) a smoother upper lip smile line and 6) release of scar constractures at the mouth corners.
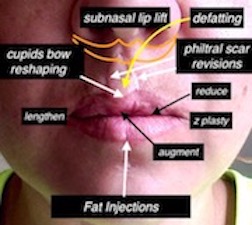
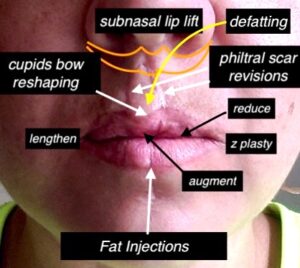 In a single lip reshaping surgery the overall plan was to treat all upper lip issues with a variety of techniques. The most significant were a subnasal lip lift, philtral scar revisions, prolabial defatting, cupid’s bow reshaping, fat injections to upper lip, smile line mucosal excisions and corner of mouth releases.
In a single lip reshaping surgery the overall plan was to treat all upper lip issues with a variety of techniques. The most significant were a subnasal lip lift, philtral scar revisions, prolabial defatting, cupid’s bow reshaping, fat injections to upper lip, smile line mucosal excisions and corner of mouth releases.

 All aforementioned lip techniques were done in a single procedure under general anesthesia with an improved upper lip shape.
All aforementioned lip techniques were done in a single procedure under general anesthesia with an improved upper lip shape.
Surgical lip techniques are interchangeable. Aesthetic lip reshaping borrows from reconstructive techniques and reconstructive lip surgery occasionally borrows from aesthetic techniques. Having a facile knowledge of both allows for a comprehensive approach to the most complex of lip revisional surgeries.
Case Highlights:
1) Complex lip reconstructions that involve a cross lip flap whether for congenital deformities or trauma introduces new unscarred tissue that will need to be molded into a better shape with subsequent revisions.
2) In cross lip flaps the transferred lip tissue may be short of the nasal base leaving a long upper lip with an unaesthetic shape to the philtrum.
3) Secondary lip revisions borrow from both reconstructive (scar revision techniques) and aesthetic procedures (subnasal lip lift, smile line reduction, fat injections) to create an improved upper lip shape.
Dr. Barry Eppley
Indianapolis, Indiana