

Background: Chin augmentation is a commonly performed aesthetic facial procedure for which an implant offers a simple solution. While effective for some the dissatisfaction with chin implant surgery is not insignificant. Many a chin implant have been successfully placed, as defined by a non-infected postoperative course (surgical success), but the patient did not achieve their desired aesthetic result. (aesthetic failure)
While the shape and size of a chin implant is critical to its aesthetic success, surgical placement becomes an equal contributor to its outcome. The best selected implant for the patient’s needs becomes adversely affect if it is placed asymmetrically or too high or too low on the bone. But you can back up these factors further by asking an initial question as to whether an implant was the best choice for the patient’s chin augmentation needs.
This brings one back to the very initial consultation/evaluation where the diagnosis/goals should be first established before the treatment is chosen. The patient may want an implant and the surgeon may be inclined to do an implant. But without some visual discussion and computer imaging to define the patient’s goals how can one accurately match the surgery needed that can come closest to reaching those goals? This is the fundamental flaw that I see all the time in unsatisfactory facial reshaping procedures including chin augmentations.

 Case Study: This young male had undergo a previous submental chin implant for his desired chin augmentation procedure. He believed it to be a 5mm extended silicone chin implant. He also had Kybella injections, five of them done afterwards. He viewed the results as not making much of a difference. By palpation the chin implant could be felt to be on the underside off his chin. (primarily vertical lengthening) Bay doing computer imaging his desired chin augmentation changes was a 12mm horizontal change
Case Study: This young male had undergo a previous submental chin implant for his desired chin augmentation procedure. He believed it to be a 5mm extended silicone chin implant. He also had Kybella injections, five of them done afterwards. He viewed the results as not making much of a difference. By palpation the chin implant could be felt to be on the underside off his chin. (primarily vertical lengthening) Bay doing computer imaging his desired chin augmentation changes was a 12mm horizontal change
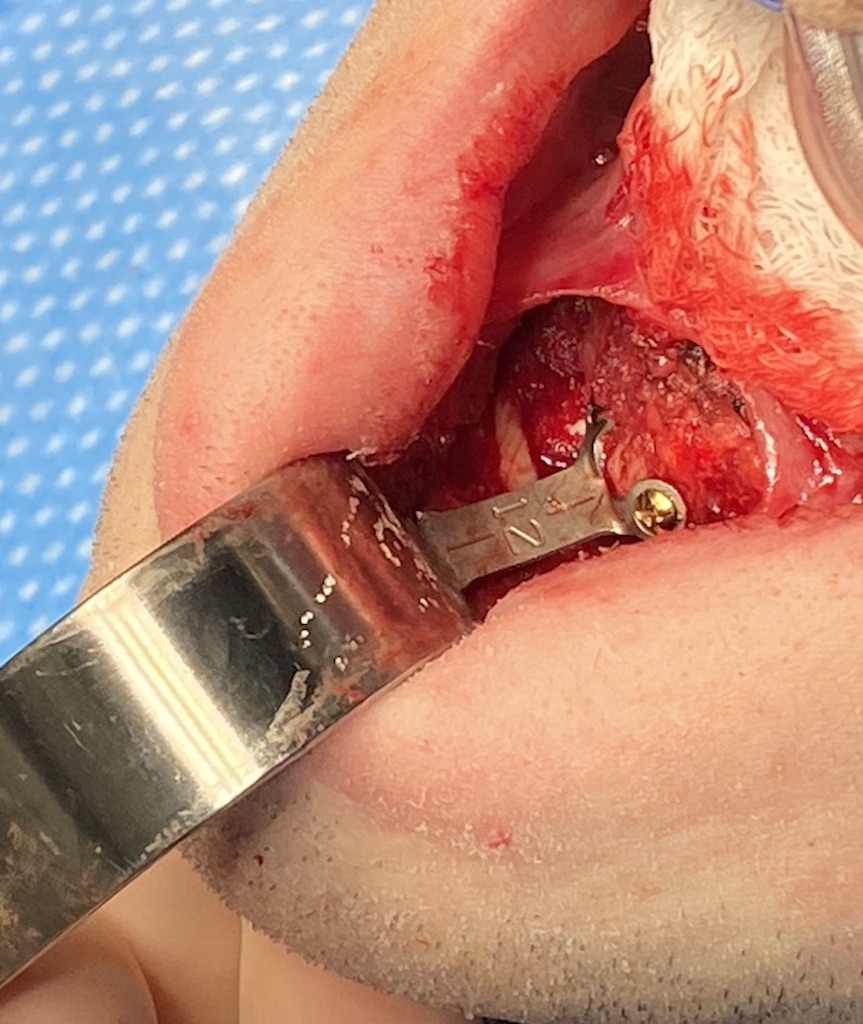
Under general anesthesia and through an intraoral approach the small chin implant located on the bottom side of the chin bone was removed and replaced with a 12mm horizontal advancing sliding genioplasty. Then going through the existing submental scar ausbmentoplasty was performed consisting of supraplatysmal liposuction, direct subplatysmal defatting and midline platysma muscle plication.

 His 6 week results showed the effects of skeletal expansion with underlying fat removal and muscle plication.
His 6 week results showed the effects of skeletal expansion with underlying fat removal and muscle plication.
While implants for chin augmentation may seem like a logical go to for treatment how would you know if you first did not establish the patient’s desired dimensional changes? Based on his determined image goals, done after the first procedure, is became clear that an implant was never going to be ale to achieve his chin augmentation goals. When you combine that with a fuller face and thick neck skeletal expansion is always going to have a better lower facial reshaping effect. The submentoplasty helps but it is just a complement to the change in chin projection caused by the sliding genioplasty.
Key Points:
1) Chin implants can aesthetically fail because of their size and placement location on the chin bone…of which the most common reason is failure to preoperatively assess the patient’s goals.
2) In fuller male faces a bony genioplasty may offer an improved aesthetic result over an implant as it more effectively pulls out the lowe rthird of the face.
3) The most effective reshaping procedure for the fuller neck patient is submentoplasty which removes maximum fat and tightens up the platysmal muscle in the midline.
Dr. Barry Eppley
World-Renowned Plastic Surgeon