


Background: Pectus excavatum is a well known congenital chest deformity that when severe enough justifies surgical correction. The historic operation is the Ravitch procedure introduced back in the early 1950s. It has become improved and is now for some time been performed as the modified Ravitch procedure in which the sternum and surrounding structures are exposed by a midline incision, abnormal cartilages removed and the sternum reshaped and elevated into a more normal position. Holding the sternum out, often with a metal bar, while the rib cartilages grow back to it is key to the long term result.
Despite the best modified Ravitch surgery being performed a certain percentage of such treated patients with have some residual sternal depression that remains as an older adult. Such secondary sternal contouring is not done by further bone or cartilage reshaping. This requires augmentation on top of the sternal ‘valley’ which can usually only be done by an implant approach. Injection fat grafting is only effective for the smallest of sternal depressions and those that only have an inferior/xiphoid depression.
When designing a sternal implant a custom implant approach is needed. This can be done by the historic moulage technique or by using 3D CT scan to design the implant. Each sternal implant design approach as its advantages and disadvantages. The moulage technique requires some skill in working with the moldable polymer during the preoperative impression visit and, more importantly, an understanding that intraoperative modification of the implant will probably be needed. How much polymer to apply and how to shape it for the desired external contour result is a learned skill that is not infallible.
 Case Study: This young male had a severe pectus excavated chest deformity treated by a modified Ravitch procedure. As a young adult he had an aesthetically bothersome residual sternal depression, greatest on the lower half of the sternum, with well healed midline vertical incision.
Case Study: This young male had a severe pectus excavated chest deformity treated by a modified Ravitch procedure. As a young adult he had an aesthetically bothersome residual sternal depression, greatest on the lower half of the sternum, with well healed midline vertical incision.

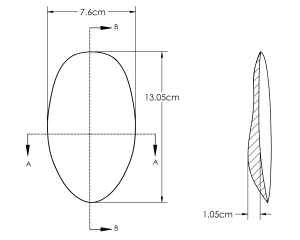 Using a self-polymerizing moulage technique, a sternal implant was fashioned. Once the polymer was set it was scanned into a computer design from which the implant was fabricated.
Using a self-polymerizing moulage technique, a sternal implant was fashioned. Once the polymer was set it was scanned into a computer design from which the implant was fabricated.
 Under general anesthesia the midline sternal incision was opened and it was found the pectorals major muscles completed covered the sternum. They were split in the midline and the depressed sternum out to all of the costal cartilages were exposed. The pectoralis minor muscle was left intact. Multiple raised and irregular costochondral junctional areas were encountered.
Under general anesthesia the midline sternal incision was opened and it was found the pectorals major muscles completed covered the sternum. They were split in the midline and the depressed sternum out to all of the costal cartilages were exposed. The pectoralis minor muscle was left intact. Multiple raised and irregular costochondral junctional areas were encountered.
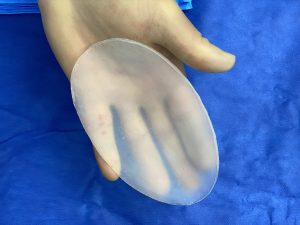
 The custom sternal implant was opened and multiple trial fits done, with reductive modifications, until a good fit was obtained. A good fit is evident when the footprint of the implant fits while being able to close the muscle over it without undue tension…and the sternal contour either looks flat or slightly depressed. (but never raised)
The custom sternal implant was opened and multiple trial fits done, with reductive modifications, until a good fit was obtained. A good fit is evident when the footprint of the implant fits while being able to close the muscle over it without undue tension…and the sternal contour either looks flat or slightly depressed. (but never raised)

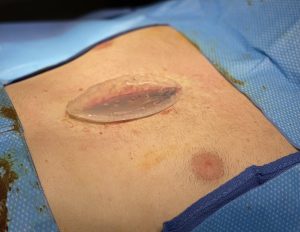
 After placing over the implant the pectorals muscle was closed over the entire implant with an additional two closure up through the skin with a resorbable subcuticular skin closure.
After placing over the implant the pectorals muscle was closed over the entire implant with an additional two closure up through the skin with a resorbable subcuticular skin closure.





 His two month postoperative showed a contour improvement of the sternum which looked perfectly natural and a midline sternal scar that looked better than the original scar.
His two month postoperative showed a contour improvement of the sternum which looked perfectly natural and a midline sternal scar that looked better than the original scar.
Case Highlights:
1) Early pectus excavatum surgery often provides good sternal-chest reshaping but residual sternal depressions are not uncommon.
2) A custom sternal implant can secondarily improve residual aesthetic sternal depressions. One method of implant fabrication is a moulage technique.
3) Even in custom sternal implant techniques intraoperative modification of some of the implant dimensions may be needed for optimal fit.
Dr. Barry Eppley
Indianapolis, Indiana