

Background: The ‘debate’ between an implant and the sliding genioplasty for chin augmentation is an historic one and is often influenced by surgical specialty and patient preference. This debate can be largely irrelevant in modest chin augmentations where their aesthetic effects are more similar. But their aesthetic benefits begin to differ when the anatomic makeup of the chin deficiency and the neck tissues become less favorable or more severe.
Larger chin deficiencies and fuller neck tissues pose different challenges for good aesthetic results. As the horizontal chin deficiency reaches double digits the benefits of a chin implant decrease with a larger implant load and less influence beyond changes to the frontal projection of the soft tissue chin pad. In addition in larger chin deficiencies the slope of the front edge of the chin can slant backwards which can make the chin implant create undesired vertical elongation.
In chin augmentations with submental fullness a chin implant with submental liposuction is a common and often very successful strategy. But as the neck tissues become fuller fat removal at the supraplatysmal level may not be enough particularly if prior defatting attempts have been done. (E.g., Kybella injections) Like the sliding genioplasty is to an implant in larger deficiencies a submentoplasty is to liposuction in fuller necks.
Case Study: This male present for chin augmentation with a prior history of a chin implant and a postoperative series of Kybella injections. Neither produced much of a change. He knew that the chin implant was a 5mm conform implant placed through a submental incision. Computer imaging and measurements looked at how much more chin augmentation would he want…assuming he was getting the full 5mms projection from the existing chin implant. It was determined that he wanted 8 to 10mms more projection. From a neck standpoint I felt that liposuction alone was not ideal and we agreed on a submentoplasty technique.
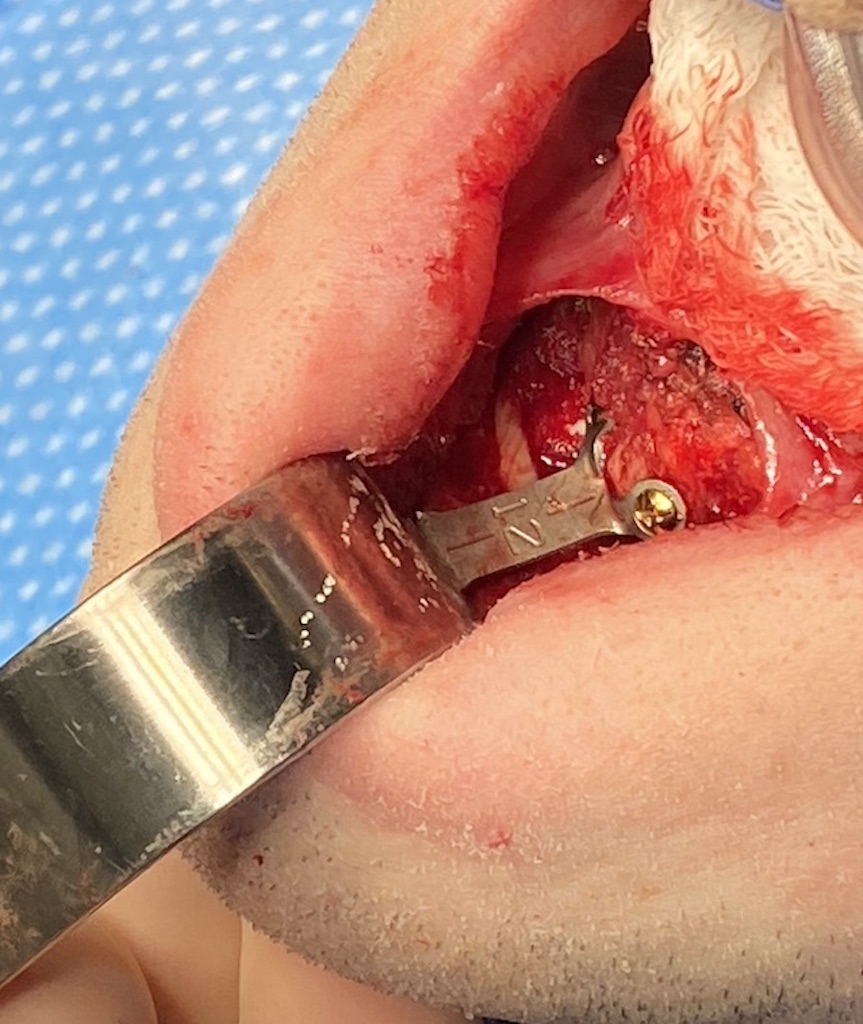
 Under general anesthesia and through an intraoral incision dissection was carried down to bottom of the chin. There the implant was found on the bottom edge of the bone with double screw fixation and removed. Based on its position it was providing little chin augmentation benefit.
Under general anesthesia and through an intraoral incision dissection was carried down to bottom of the chin. There the implant was found on the bottom edge of the bone with double screw fixation and removed. Based on its position it was providing little chin augmentation benefit.

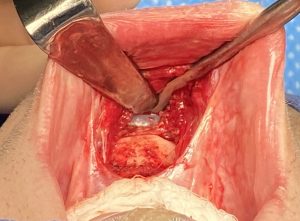
 A 12mm sliding genioplasty was performed with 5cc of cadaveric bone chips placed into the bony step deformity to help recontour the shape of the bone.
A 12mm sliding genioplasty was performed with 5cc of cadaveric bone chips placed into the bony step deformity to help recontour the shape of the bone.

 Through this existing submental incision from his prior chin implant small cannula liposuction was initially performed followed by direct defatting. By splitting open the platysma in the midline subplastysmal fat was removed and a platysma plication done.
Through this existing submental incision from his prior chin implant small cannula liposuction was initially performed followed by direct defatting. By splitting open the platysma in the midline subplastysmal fat was removed and a platysma plication done.

 His intraoperative before and after already showed the profile improvement.
His intraoperative before and after already showed the profile improvement.
Anatomic challenges posed by a short chin and fuller neck are never going to be optimally improved by a minimalistic approach. A small chin implant and Kybella injections are going to be inadequate no matter how well they are done. When a significant chin deficiency exists with a fuller neck it is the bone that must be pulled forward to help the submental area of the neck. In that same regard liposuction alone will not produce the best neck contour change. A submentoplasty does not add much to the recovery but is more effective at fat removal as well as tightens the muscle right at the cervicomental angle.
Key Points:
1) Short chins with fuller necks are often not a good candidate for a chin implant and minimalistic neck defatting techniques.
2) A sliding genioplasty has the advantage in fuller/thicker necks of helping to stretch the tissues out from the muscle attachments on the back side of the advanced chin bone.
3) A submentoplasty offers the best potential improvement in thick tissued necks and combined with a sliding genioplasty offers the optional profile improvement.
Dr. Barry Eppley
World-Renowned Plastic Surgeon