


Background: Chin implants in females are commonly performed but must take into consideration how their aesthetic objectives differ from men. Chin augmentation is often made too dimensionally simplistic by just looking at the patient’s profile and making all decisions based on how much projection is being created. The change that occurs in the frontal view that results from the profile change must also be anticipated.
Most chin implant styles are extended, meaning they have extension or wings which are intended to make the augmented chin blend smoothly into the jawline behind it. Snd they do this very well but there is a tradeoff for doing so….it makes the chin wider. The very thin extensions on this chin implant style, even though only a few millimeters and fading into a feather edge, can make the chin wider when seen in the front view. While aesthetically acceptable in men, such increased chin width is not in women unless they have specifically asked for it.
A very appealing aspect of placing a chin implant in a female is the intraoral approach. Avoiding a submental scar is a good goal for any patient but it comes with its own potential liabilities. Because the incision is far ‘removed’ from where the implant needs to be placed (lower end of the chin bone) failure to use screw fixation will always result in implant malposition. The implant immediately slides upward as soon as the incision is closed, ending in a higher position on the bone than where its maximal augmentation effect can be achieved. But a less appreciated liability is in the patient who has pre-existingmentalis strain and lower lip incompetence. To place an intraoral implant the mentalis muscle must be transacted near its origin to access the lower end of the chin bone. While the muscle is put back together during closure the creation of scar tissue and the placement of an artificial block of material behind the muscle does not usually improve the mentalis strain. Often a persistent tightness of the chin occurs and the feeling that an implant is present can occur.
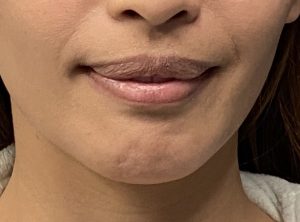
Case Study: This female has a chin implant placed intraorally one year previously. Its amount of horizontal projection was unknown but its extended style was. It was known to be secured with multiple screws with one screw broken off as told her by her surgeon. While she liked the increased projection achieved in profile she did not like that her chin became wider. Equally relevant was that the chin implant never felt natural. Her chin remained tight after the swelling resolved and her pre-existing mentalis strain was not improved. She opted for chin implant removal and replacement with a sliding genioplasty. Aesthetically she desired a few more millimeters of horizontal projection and a less wide chin appearance.

 Under general anesthesia and through her existing intraoral scar/incision, the chin implant was exposed. The four screws placed during is insertion were taken out and the chin implant removed. Its extended impalant style could be appreciated.
Under general anesthesia and through her existing intraoral scar/incision, the chin implant was exposed. The four screws placed during is insertion were taken out and the chin implant removed. Its extended impalant style could be appreciated.

 Because of the excellent midline positioning of the chin implant full-thickness bone cuts were made at the upper level of the implant pocket on both sides. The bone was downfractured and advanced 8mms using a central fixation plate and screws. The bony step off created was filled with 5ccs of tissue back bone chips.
Because of the excellent midline positioning of the chin implant full-thickness bone cuts were made at the upper level of the implant pocket on both sides. The bone was downfractured and advanced 8mms using a central fixation plate and screws. The bony step off created was filled with 5ccs of tissue back bone chips.

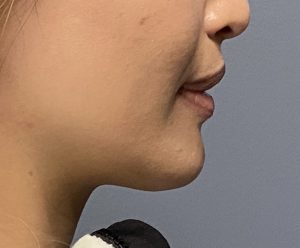
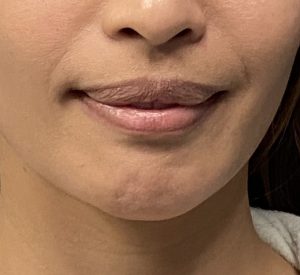 Her immediate (one day postop) results showed the increased chin projection and, even in the face of swelling, a chin that was less wide. The fate of her mentalis strain awaits a full recovery.
Her immediate (one day postop) results showed the increased chin projection and, even in the face of swelling, a chin that was less wide. The fate of her mentalis strain awaits a full recovery.
 Besides the usual lesson of be aware of the chin widening effect of most standard chin implants in females, the other lesson is that of the effects of the intraoral approach for chin implants in the presence of mentalis strain and lower lip incompetence. Such symptoms may not be improved and new symptoms of chin pad tightness and an unnatural feeling of the chin may occur. One can have a debate about whether an implant or moving the chin bone forward offers a better chance at symptomatic improvement but the risks of increased symptoms is probably less when the implant placed is assistive to the operation and not the whole operation itself.
Besides the usual lesson of be aware of the chin widening effect of most standard chin implants in females, the other lesson is that of the effects of the intraoral approach for chin implants in the presence of mentalis strain and lower lip incompetence. Such symptoms may not be improved and new symptoms of chin pad tightness and an unnatural feeling of the chin may occur. One can have a debate about whether an implant or moving the chin bone forward offers a better chance at symptomatic improvement but the risks of increased symptoms is probably less when the implant placed is assistive to the operation and not the whole operation itself.
Case Highlights:
1) Chin implants can be associated with persistent chin pad tightness when placed intaorally or when pre-existing lower lip incompetencce/mentalis strain exists.
2) Extended or winged chin implants when used in females commonly makes the chin have an undesirable wider appearance.
3) Symptomatic chin implants are usually improved by a sliding genioplasty replacement, particularly when increased horizontal projection is needed.
Dr. Barry Eppley
Indianapolis, Indiana