


Background: The chin implant is viewed as a simple surgery with no significant anatomic issues for its placement. But this often viewed concept is inaccurate as it fails to appreciate that an important element of making the implant pocket is release of some or all of the osteoligamentous attachments in making the suboperosteal pocket. If not adequately released implant malpositon will occur when using any winged chin implant style. (extended anatomic designs)
While release of the ligaments are a necessity for implant placement there are potentially adverse sequelae should the implant ever be removed. Contrary to popular perception of many surgeons the chin is not simply going to shrink back down and return to normal. It can’t as the ligaments can not reattach once they have been released. The capsule on the outer surface of the implant on the tissue side slides off the underlying capsule of the bone once the implant spacer is removed between the two. This causes some degree of chin road sagging/excess. This can be very minor and aesthetically irrelevant to the patient. Or it can be more significant and problematic to them.
Soft tissue chin pad excess after implant removal is typically most pronounced when smiling. This causes a new/unnatural roll under the chin and, in more significant cases, may display a pulldown of the chin pad. (hyperdynamic chin pad ptosis) The only effective treatment is removal of a portion of the chin pad and tightening it under the chin bone. Techniques such as intraoral suspensions and chin pad liposuction will universally fail to provide any improvement.
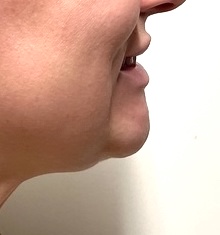
 Case Study: This female had a prior history of a chin implant placed that she disliked and was subsequently removed after several months. As a result she developed some chin pad excess which became most prominent when she smiled. It was subsequently treated by liposuction which not surprisingly failed to provide any improvement. (actually made it more ball-shaped than before. Botox and fillers also failed to make any headway on its resolution.
Case Study: This female had a prior history of a chin implant placed that she disliked and was subsequently removed after several months. As a result she developed some chin pad excess which became most prominent when she smiled. It was subsequently treated by liposuction which not surprisingly failed to provide any improvement. (actually made it more ball-shaped than before. Botox and fillers also failed to make any headway on its resolution.

 Under general anesthesia a submental excision technique was used in which the length of the incision was going to be limited to no wider than the sides of the upside down triangle formed by the junction of mouth corner-jawline lines. A full thickness wedge of skin, fat and and muscle was removed from the inferior chin pad. The submental area below the incision was directly defatted and thinned so the thickness of the chin pad and neck at the incisional closure matched.
Under general anesthesia a submental excision technique was used in which the length of the incision was going to be limited to no wider than the sides of the upside down triangle formed by the junction of mouth corner-jawline lines. A full thickness wedge of skin, fat and and muscle was removed from the inferior chin pad. The submental area below the incision was directly defatted and thinned so the thickness of the chin pad and neck at the incisional closure matched.

 The submental approach for chin pad excess offers improvement in the shape of the chin by combining excision and tightening along the inferior border of the chin bone. Almost always the thickness of the submental tissues below the initial incision needs to be done for the best profile result. While there is a scar tradeoff for the elimination of the hyperdynamic chin pad it is the only solution for what has become a tissue excess/sagging problem from loss of the soft tissue ligamentous attachments. One key to a good submental scar is to keep its length limited ands the preoperative markings provide a guideline as how to do so.
The submental approach for chin pad excess offers improvement in the shape of the chin by combining excision and tightening along the inferior border of the chin bone. Almost always the thickness of the submental tissues below the initial incision needs to be done for the best profile result. While there is a scar tradeoff for the elimination of the hyperdynamic chin pad it is the only solution for what has become a tissue excess/sagging problem from loss of the soft tissue ligamentous attachments. One key to a good submental scar is to keep its length limited ands the preoperative markings provide a guideline as how to do so.
Case Highlights:
1) The soft tissue chin pad after implant removal may not return to its preoperative shape due to loss of its osteoligamentous attachments
2) Soft tissue chin pad excess can only be improved by an excisional technique.
3) One of the keys to soft tissue chin pad excision is to prevent its lateral extent from crossing the mouth corner-jawline triangle border.
Dr. Barry Eppley
World-Renowned Plastic Surgeon