


Background: The shape of the chin in all views is a combination of the the bone and the enveloping soft tissue chin pad. Typically there is a confluent appearance of the chin as the soft tissue chin pad is tightly adherent to the bone through ligamentous and muscular attachments. But the there are certain clinical situations where the soft tissue chin pad becomes separated from the bone and hangs off of it in varying degrees and is known as chin ptosis. (e.g., chin implant removal, intraoral chin bone reduction, significant alveolar bone loss) This lack of attachment of the soft tissue and bone is seen at rest and can occur regardless of the degree of chin projection present.
A unique form of chin ptosis presents in a dynamic fashion or when one is smiling known as hyperdynamic chin ptosis. The soft issue chin pad pulls down over the bone when the sides of the mouth corners elevates the chin pad. This appears as a roll of skin/soft tissue that hangs below the inferior border of the chin bone. From the front view the chin lengthens and the shape of the chin pad either appears square or v-shape. In my experience I have only seen hyperdynamic chin ptosis in chin that either have normal projection or slightly excessive bony projection.
The interesting question is why does hyperdynamic chin ptosis occur when the chin is otherwise normal at rest. Since it is a dynamic event it is muscle related. Once of the major muscles of the chin is the mentalis muscle. This paired central muscle of the lower lip originates superiorly on the bone and inserts below the inferior portion of the chin bone into the soft tissues over and under the chin. Its action on contraction is an upward and inward movement of the soft tissue chin pad which then raises the central portion of the lower lip. As a result hyperdynamic chin ptosis, like any other over active muscle of facial expression, can be partially or completely alleviated by neuromuscular weakening agents (e.g., Botox) albeit temporalily.

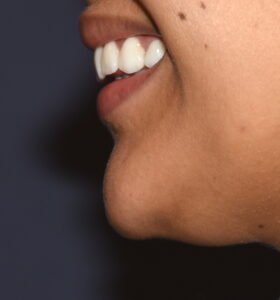

 Case Study: This young female presented with concerns of an aesthetically undesired hyperdynamic chin ptosis and a chin that was too pointy at rest.
Case Study: This young female presented with concerns of an aesthetically undesired hyperdynamic chin ptosis and a chin that was too pointy at rest.



 Under general anesthesia the markings for a submental chin resection approaches are based on a limited crescent incision that stays well within vertical lines dropped down from the corners of the mouth. Through this submental incision the shape of the chin bone was changed from a strong pointy shape to a rounder flatter shape.
Under general anesthesia the markings for a submental chin resection approaches are based on a limited crescent incision that stays well within vertical lines dropped down from the corners of the mouth. Through this submental incision the shape of the chin bone was changed from a strong pointy shape to a rounder flatter shape.
 The soft tissue chin pad was then pulled down over the reshaped chin bone, soft tissue excess removed and a submental chin tuck completed. The mentalis muscle is tacked down under the chin bone to the bony periosteum and the geniohyoid muscle.
The soft tissue chin pad was then pulled down over the reshaped chin bone, soft tissue excess removed and a submental chin tuck completed. The mentalis muscle is tacked down under the chin bone to the bony periosteum and the geniohyoid muscle.
Hyperdynamic chin ptosis is multifactorial in origin but an overactive mentalis muscle appears to be the primary cause. Many such women so affected often have a borderline prominent chin bone and/or a pointy chin shape that affects how the soft tissue chin pad appears when smiling. A submental tuck with or without bone reshaping offers an effective surgical approach.
Case Highlights:
1) Hyperdynamic chin ptosis is different than traditional chin ptosis as it appears only when one is smiling. (dynamic motion)
2) Hyperdynamic chin ptosis typically appears as a near square shaped deformation of the soft tissue chin pad which has an edge that drops below the static inferior chin line.
3) A submental chin tuck, usually with some bone reduction to allow space for the tuck, can effectively treat many cases of hyperdynamic chin ptosis.
Dr. Barry Eppley
Indianapolis, Indiana