

Background: The well known sliding genioplasty is a versatile chin reshaping procedure due to its capability of multidimensional movements. While most known for ‘sliding’ the chin bone forward (increased horizontal projection) it is capable of changing the vertical height of the chin (longer or shorter) as well as its width. This capability of change is why its use is an integral part of v-line jaw reshaping surgery.
The ability to make the downfractured chin bone so dimensionally changeable is how it is put back together and held there. Plate and screw fixation allows the bone to be placed and/or reassembled in a variety of ways that are stable and allows for uncomplicated bone healing. Long ago has the use of wires been replaced by these plate and screws due to their versatility. Another less commonly used chin fixation method are bicortical screws which, while effective for healing, limits the chin dimensional changes by how the screws have to pass through the chin bone segment.
When performing the sliding genioplasty in women, similar to chin implants, a key aesthetic issue is to avoid over correction. Unlike men the horizontal chin projection in women should not come as far forward as the classic vertical line dropped down from the lips…as that will almost always been seen as too much
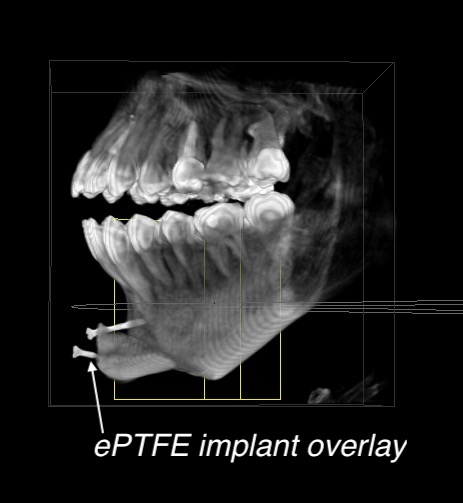
 Case Study: This young female with a fairly short chin desired a more tapered jawline shape. To try and achieve this jawline look she underwent a surgery by another surgeon consisting of Goretex jaw angle implants and a sliding genioplasty of 10mm forward movement and significant vertical shortening with a single bicortical screw fixation. Goretex implants were also added to the front of the chin bone with midline screw fixation. Her postoperative course was complicated by a left jaw angle implant infection, concerns that her chin was over corrected and a tightness in the labiomental fold that did not resolve with prolonged healing. A 3D CT scan shows the chin bone position, screws and the ghost image of how thick the Goretex chin implant overlay was.
Case Study: This young female with a fairly short chin desired a more tapered jawline shape. To try and achieve this jawline look she underwent a surgery by another surgeon consisting of Goretex jaw angle implants and a sliding genioplasty of 10mm forward movement and significant vertical shortening with a single bicortical screw fixation. Goretex implants were also added to the front of the chin bone with midline screw fixation. Her postoperative course was complicated by a left jaw angle implant infection, concerns that her chin was over corrected and a tightness in the labiomental fold that did not resolve with prolonged healing. A 3D CT scan shows the chin bone position, screws and the ghost image of how thick the Goretex chin implant overlay was.

 Under general anesthesia her infected jaw angle implants were initially removed. In looking at the vestibular incision in the chin a opening in the incision line was seen with fluid egress. This track as followed down to the Goretex onlay chin implants which were removed.
Under general anesthesia her infected jaw angle implants were initially removed. In looking at the vestibular incision in the chin a opening in the incision line was seen with fluid egress. This track as followed down to the Goretex onlay chin implants which were removed.
 The single midline bicortical screw was removed and an osteotomy was preformed to downfracture the previously advanced chin segment. It was then setback from 10 to 6mms and fixed with a step plate and screws.
The single midline bicortical screw was removed and an osteotomy was preformed to downfracture the previously advanced chin segment. It was then setback from 10 to 6mms and fixed with a step plate and screws.
Larger amounts of chin advancements can be done by a combined sliding genioplasty and implant overlay. In this situation the need for a partial reversal for over correction can be done by implant removal and setback osteotomy. The ratio between the two, and whether both needs to be done, depends on how much setback is needed.
Case Highlights:
1) V-line surgery typically involves some form of a sliding geniplasty which narrows the chin by either advancement or a midline wedge bone removal.
2) When the narrowness of the chin is created by a large horizontal advancement overcorrection can occur in profile…which can be secondarily treated by a subtotal sliding genioplasty reversal.
3) Large horizontal chin advancements associated with significant vertical shortening can cause labiomental fold/intraoral vestibular tightness due to soft tissue compression.
Dr. Barry Eppley
Indianapolis, Indiana