


Background: Chin augmentation by an implant or a sliding genioplasty are procedures that have a relatively low rate of infection or wound healing problems. But just because these risks are low does not mean they can not occur under the right circumstances.
One factor that can contribute to these problems is stress or pressure devascularization on the chin wound closure whether it is an intraoral or submental incision. One of the unique features of the soft tissue chin pad, like the tip of the nose, is that it is not that stretchable or elastic. It is soft tissue that is stretched over a solitary projecting point. Unlike the tip of the nose, however, the soft tissue chin pad is stretched over rigid bone or, when an augmentation is performed, a firm implant.
When the tension on the soft tissue chin pad closure is excessive the blood supply to the incision edges can become compromised and wound breakdown can occur. This occurs almost exclusively when an implant under the incision is involved. This is rare in a primary chin implant augmentation but always has to be considered when the chin tissues have been stretched out from prior surgery.
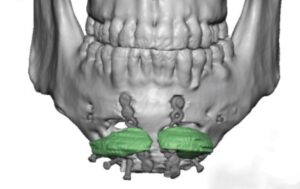
 Case Study: This male came to me with a prior chin surgery history of a vertical lengthening bony genioplasty with the placement of Medpor chin implants for horizontal augmentation. To the best I could tell Medpor implants were placed to fill the gaps created by the bony lengthening during the initial bony genioplasty surgery. Secondarily a Medpor chin implant was placed through a submental incision.
Case Study: This male came to me with a prior chin surgery history of a vertical lengthening bony genioplasty with the placement of Medpor chin implants for horizontal augmentation. To the best I could tell Medpor implants were placed to fill the gaps created by the bony lengthening during the initial bony genioplasty surgery. Secondarily a Medpor chin implant was placed through a submental incision.
 While that provided the ideal amount of vertical and horizontal chin augmentation from a dimensional standpoint, the soft tissue chin pad could not tolerate that amount of stretch and resulted in a submental wound dehiscence. The patient put considerable effort into trying to make it heal over the implant secondarily…but that did not work after one year of effort.
While that provided the ideal amount of vertical and horizontal chin augmentation from a dimensional standpoint, the soft tissue chin pad could not tolerate that amount of stretch and resulted in a submental wound dehiscence. The patient put considerable effort into trying to make it heal over the implant secondarily…but that did not work after one year of effort.

 Under general anesthesia the wound edges around the submental wound were excised. Through this opening two layers of Medpor implants were removed and their fixation screws as well as the lower half of the plates and screws from the vertical chin lengthening.
Under general anesthesia the wound edges around the submental wound were excised. Through this opening two layers of Medpor implants were removed and their fixation screws as well as the lower half of the plates and screws from the vertical chin lengthening.
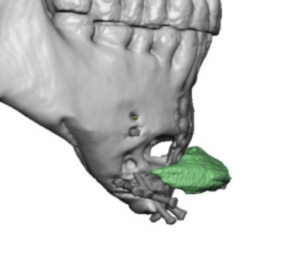
 This left a large internal wound space which, rather than letting it collapse inward as it heal and result in a significant chin deformity, it was filled with a large en bloc fat graft harvested from the abdomen.
This left a large internal wound space which, rather than letting it collapse inward as it heal and result in a significant chin deformity, it was filled with a large en bloc fat graft harvested from the abdomen.
 With a 3 x 3cm open chin pad wound, which reflected the amount of missing skin, primary closure was done over the fat graft resulting in an indentation as expected. This will require further soft tissue chin surgery to contouring/scar revision four to six months later.
With a 3 x 3cm open chin pad wound, which reflected the amount of missing skin, primary closure was done over the fat graft resulting in an indentation as expected. This will require further soft tissue chin surgery to contouring/scar revision four to six months later.
The initial goal in a chin implant wound dehiscence of a chronic nature is to create a healed infection free chin site. This requires removal of all synthetic materials including any metal. Most of the time the wound space will heal in on itself without major chin contour deformities. But in very large chin implants the internal wound space is considerable and significant chin pad contracture will occur. Placing a fat graft will help prevent such severe contracture and will not adversely affect wound closure because it is soft. (not like a hard implant)
The lessons to be learned from this case are as follows:
- When a chin implant becomes exposed immediate surgical management is needed. Few wound dehiscences can ever heal in on their own in the chin area. Tissues will not granulate and heal over a synthetic material.
- When the chin tissues have been stretched out from a prior sliding genioplasty (whether it is vertical or horizontal) be careful about stripping off the soft tissues from below and placing a large chin implant secondarily. Whether it is obvious or not the soft tissue chin pad has already been stretched out and its tolerance to such stresses are less than normal.
Case Highlights:
1) Excessive pressure on the soft tissue chin pad from an implant through a submental incision can result in postoperative wound dehiscence and implant exposure.
2) Once a chin implant has become exposed it requires immediate surgery if any chance for successful salvage is to be realized.
3) With a wound dehiscence and a chronically infected implant removal is indicated and consideration can be given to a fat graft to prevent severe wound contracture.
Dr. Barry Eppley
Indianapolis, Indiana