

Background: The forehead is the largest surface area on the face with seemingly limited distinguishing characteristics. Hair makes up its most identifiable features which are relegated to the borders with the frontal and temporal hairlines superiorly and laterally and the eyebrows inferiorly. The most recognized bony feature are the more prominent brow bones in men. While the large bony surface of the forehead does have some gender differences in its overall shape it does not usually stand out unless there are isolate protrusions or an overall asymmetry.
Aside from an overall large surface area frontal bossing, the most common smaller bony protrusions that occur on the forehead are horns (prominent frontal eminences) and osteomas. Osteomas often have a traumatic history for their development but horns have a congenital origin as the beginning location of bony forehead development in utero. Forehead asymmetries also have a congenital origin most commonly from an overall plagiocephaly. While the most severe manifestations of plagiocephaly are the flatness on one side of the back of the head there often is an ipsilateral smaller protrusion on the forehead due to the rotation of the skull.
In the male with forehead protrusions or asymmetry bony reductions can be successfully done. The most important aesthetic question however is where to place the incision to do so. In men with good frontal hairlines this is the best and most direct access to do the bony forehead reduction. But in men with frontal hairlines that are receded and have an M-shaped hairline patterns this is not a good option as linear access can not be obtained to the bony prominences.
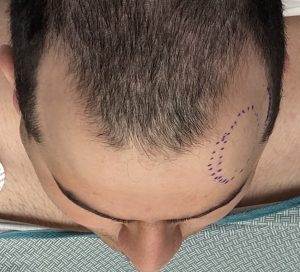 Case Study: This male was bothered by a left forehead prominence that could be adequately reduced by a burring technique. Frontal hairline incisional access was not possible given his hairline.
Case Study: This male was bothered by a left forehead prominence that could be adequately reduced by a burring technique. Frontal hairline incisional access was not possible given his hairline.

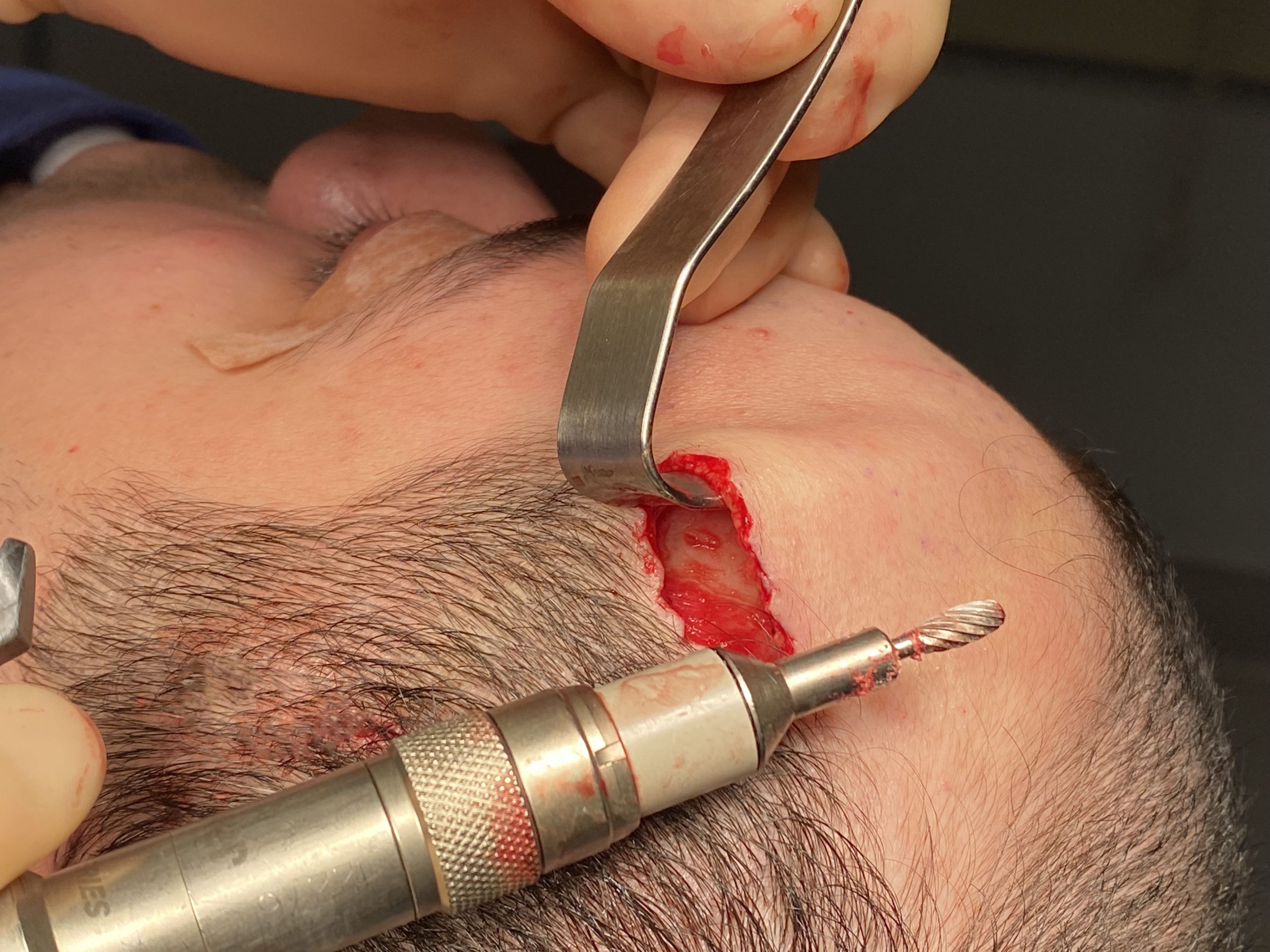
 Under general anesthesia an anterior temporal hairline incisions was made instead. Through this incision the forehead prominence was initially reduced by burring.
Under general anesthesia an anterior temporal hairline incisions was made instead. Through this incision the forehead prominence was initially reduced by burring.

 Final smoothing of the reduced forehead area was done a large skull rasping tool. Incisional closure with 6-0 plain suture produced a minimal scar line. Good reduction of the forehead prominence was achieved.
Final smoothing of the reduced forehead area was done a large skull rasping tool. Incisional closure with 6-0 plain suture produced a minimal scar line. Good reduction of the forehead prominence was achieved.

 When seen sic months later for another procedure the scar had healed so well that it was barely perceptible if at all.
When seen sic months later for another procedure the scar had healed so well that it was barely perceptible if at all.
Hairline incisions provide the most direct linear access to most forehead bony reductions. While some understandably worry about the appearance of the scar it is usually superior to any scar placed behind the hairline. As the incision gets further back in the hairline linear access is lost through a limited incisional length and now the incision must be longer…often a lot longer. It must become long enough that the enough scalp is lifted so that one can see around the bony curve of the upper forehead. This is a simple matter of geometry. As the hypotenuse gets longer (line of sight needed) the limbs of the triangle (horizontal incision length) need to be equally long.
Case Highlights:
1) Most bony forehead protrusions have a congenital origin either as isolated mounds or an overall forehead bossing.
2) The approach to the male with forehead mound protrusions must consider the incision location based on their hairline locations.
3) The anterior temporal hairline can be a good incision location for select forehead contouring in the male with a receded and distant frontal hairline.
Dr. Barry Eppley
Indianapolis, Indiana