


Background: Temporal hollowing results from lipoatrophy which can occur for a variety of reasons from aging to medical conditions. Variety methods have been used treat it, most of which are injectable, but the only permanent method are implants. Temporal implants are unique from all other aesthetic facial implants in that they are designed to augment muscle and not bone. Temporal hollowing is a soft tissue deficiency usually caused by fat loss in the muscle space
Preformed temporal implants have been developed to treat various amounts of hollowing. Two styles are available which differ in the size and shape. Style 1 temporal implants are smaller, slightly wider than tall, are used to treat lower temporal hollowing near the zygomatic arch. Style 2 temporal implants are larger, much taller than they are wide and used to fill in the entire temporal hollows from the arch to the forehead. Both styles range in thickness from 3 to 6mms.
While each temporal implant style is placed through an incision behind the temporal hairline their method of insertion differs. Style I implants can be inserted through the incision in a more linear fashion since the implant is longer (wider) than it is tall. Style 2 implants, however, can not be placed with a straight path of insertion due to their length:width ratio. Rather as they are inserted they must be turned 60 to 90 degrees to enter the vertical length of the subfacsal pocket. It is this unique path of insertion in Style 2 temporal implant that can be source of their malpositioning.
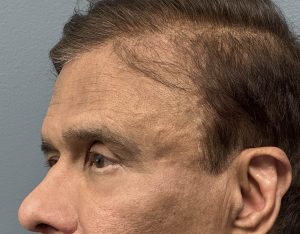
Case Study: This older male had large Style 2 temporal implants placed for long-standing lipoatrophy though an incision back in the temporal hair. He noticed malposition of the implants soon after surgery increased fullness higher up on the side of his head and increased temporal hollowing deepening above the zygomatic arch. By palpation the implants could be seen to be at a 45 degree angulation to their needed vertical orientation. On the right side the top of the implant was right under the healed incision. On the left side the bottom side of the implant was under the incision.

 Under sedation anesthesia the outline of the implants was marked and their angulated orientation could be fully visualized.
Under sedation anesthesia the outline of the implants was marked and their angulated orientation could be fully visualized.

 The incisions were opened and the implants edges immediately seen and the implants removed. When positioned externally as to how they were laying internally the degree of implant malposition could be fully appreciated.
The incisions were opened and the implants edges immediately seen and the implants removed. When positioned externally as to how they were laying internally the degree of implant malposition could be fully appreciated.
 New smaller temporal implants were selected and modified for placement. (vertically shortened as is often necessary) The pockets were extended both inferiorly and superiorly by blind capsulotomies for improved implant orientation.
New smaller temporal implants were selected and modified for placement. (vertically shortened as is often necessary) The pockets were extended both inferiorly and superiorly by blind capsulotomies for improved implant orientation.

 The new implants were inserted and placed on a more vertical orientation. To prevent them from sliding back into the old pocket/orientation the unneeded part of the pocket closure to the incision was closed down by a percutaneous bolster technique.
The new implants were inserted and placed on a more vertical orientation. To prevent them from sliding back into the old pocket/orientation the unneeded part of the pocket closure to the incision was closed down by a percutaneous bolster technique.
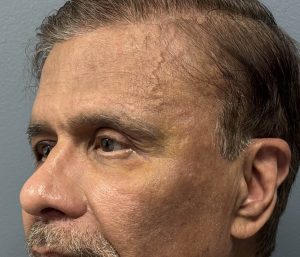

 The bolsters stayed in place for 3 days to help the implants maintain their desired vertical orientation. The improvement in the temporal augmentation effect could be appreciated. There is still some swelling and a bit of bruising but the wide upper head and the deeper lower temporal hollows are gone.
The bolsters stayed in place for 3 days to help the implants maintain their desired vertical orientation. The improvement in the temporal augmentation effect could be appreciated. There is still some swelling and a bit of bruising but the wide upper head and the deeper lower temporal hollows are gone.
Implant malpositions are almost always the result of how they were placed, not because they moved after placement…contrary to what most surgeons and patients think. This would be particularly true in large implants which occupy a comparatively small anatomic area. Successful implant outcomes depend on three factors; proper implant size, adequate pocket dissection and proper implant orientation. Failure to achieve all three will result in an unsuccessful aesthetic outcome.
Key Points
1) The permanent method of temporal augmentation is subfascial implants.
2) The extended temporal implant must be aligned vertically between the bony temporal line of the forehead and the zygomatic arch at an angle to the temporal incision location
3) Oversized and malpositioned temporal implants can be replaced with efforts made to prevent the new implant from sliding back into the old pocket.
Dr. Barry Eppley
World-Renowned Plastic Surgeon