

Background: Chin reduction is a very different operation than chin augmentation. Expansion of a projecting structure is far easier to successfully accomplish than a reduction of it. The best illustration of this difference is the corollary of aesthetic breast surgery. The use of a breast implant expands the overlying soft tissues and soft tissue excess is not usually a problem. Conversely reducing an enlarged breast mound is a very different matter. Size reduction can only be achieved by removing support (breast tissue) which then requires reduction of the overlying skin which can not shrink down on its own around this reduced support.
Chin reduction has historically been looked at as a bone problem. Different approaches to this bone excess have been done including various methods of bone shaving and osteotomies. Osteotomies technique included style reverse sliding genioplastigs and the more contemporary t-shaped genioplasty. While a sliding genioplasty works well for advancing the chin bone, sliding it in reverse does not do as well. The attached soft tissues are pushed back and into the submental region creating increased fullness. The end of the genioplasty wings drop below the interior border cresting prominent bone bumps.
Chin reduction by shaving is often done intraorally. To do so wide stripping of the soft tissues needs to be done for access to the bone. Between the loss of bone support and the tissue detachments from the bone the risk of chin ptosis excess is high. This risk is lessened when the shaving is done from a submental approach where the superior soft tissue support is maintained and any loose tissue or redundancies can be removed during closure.
Case Study: This female has two prior efforts at chin reduction surgery. An initial reverse sliding genioplasty was done followed by a submental approach where the exact technique used was unknown. She was left with a wide/square chin shape, bone ‘spurs along the inferior border being the chin and soft tissue redundancies at the ends of the submental scar.

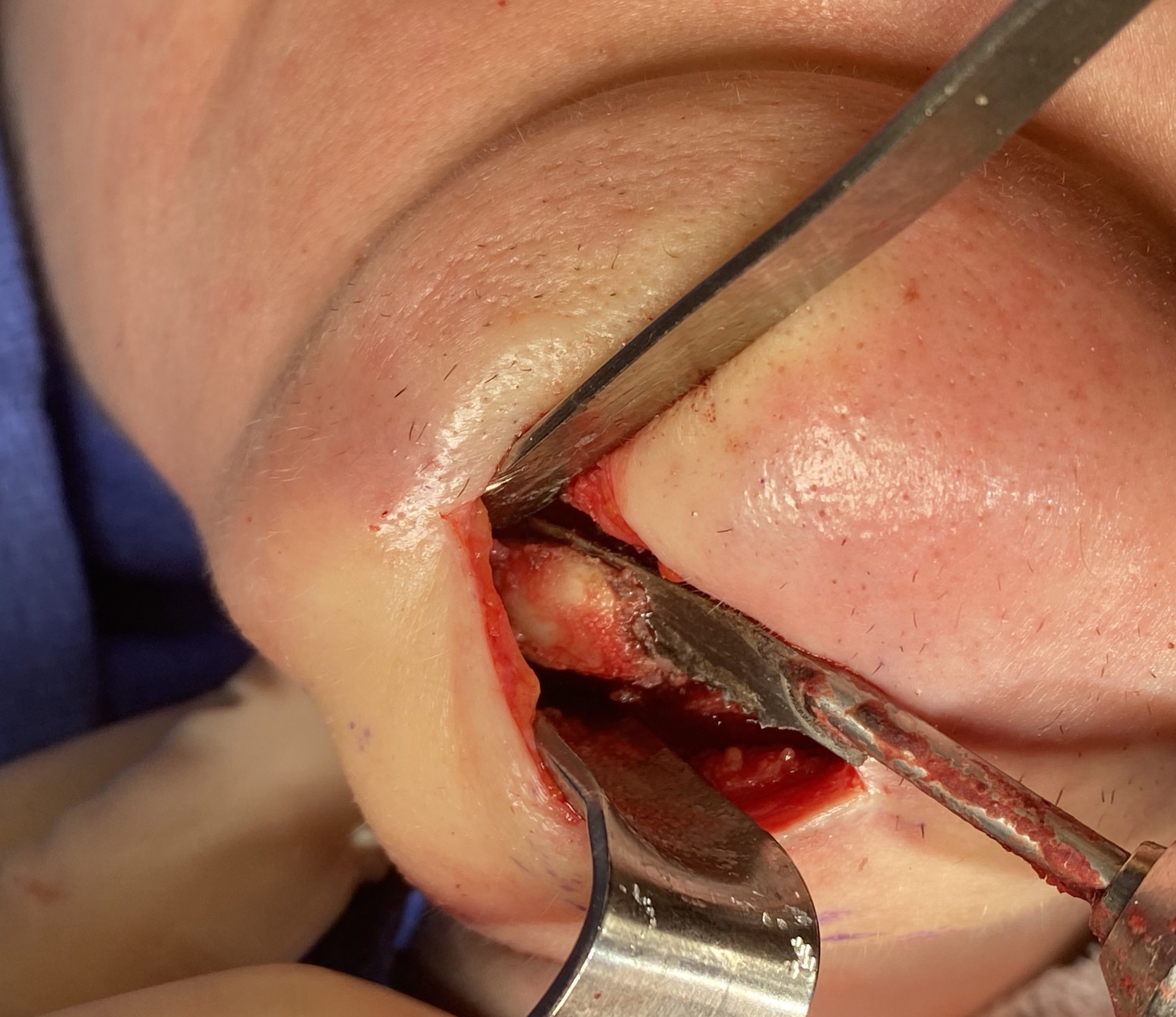
 Under general anesthesia her existing submental incision was opened to reveal a very square chin bone shape. Two spikes of bone were identified further back along the inferior border at the back end of the prior sliding genioplasty. Using a reciprocating saw the inferior border was smoothed out and rectangular wedges of bole were removed from each chin corner. This made the chin have a profound V shape which is necessary to make a more narrow chin.
Under general anesthesia her existing submental incision was opened to reveal a very square chin bone shape. Two spikes of bone were identified further back along the inferior border at the back end of the prior sliding genioplasty. Using a reciprocating saw the inferior border was smoothed out and rectangular wedges of bole were removed from each chin corner. This made the chin have a profound V shape which is necessary to make a more narrow chin.
 A crescent shaped of soft tissue with a small vertical wedge was removed from under the chin creating a t-shaped skin closure and tissue tightening around the reduced chin bone.
A crescent shaped of soft tissue with a small vertical wedge was removed from under the chin creating a t-shaped skin closure and tissue tightening around the reduced chin bone.

 Her intraoperative results showed a profound chin shape change that was more consistent with a female lower third of the face.
Her intraoperative results showed a profound chin shape change that was more consistent with a female lower third of the face.
When prior chin reductions are inadequate the definitive corrective procedure usually requires a submental technique. From this approach with bone and soft tissue excesses can be managed with a tighter redrawing of the soft tissue chin pad over the reduced chin bone.
Case Highlights:
1) A reverse sliding genioplasty is not an effective technique for chin reduction and adversely affects chin shape and disrupts the inferior border of the jawline.
2) Most unsuccessful chin reductions result from failure to adequately reduce the bone shape or completely overlook the need for soft tissue reduction as well.
3) The submental chin reduction permits a combination of bony and soft tissue reductions.
Dr. Barry Eppley
Indianapolis, Indiana