

Background: Amongst the numerous types of implants for aesthetic body augmentation the arms are the least commonly performed. Breasts, buttock, pectoral and calf implants make up the majority of augmentations while arm implants (shoulder, biceps, triceps) are done by comparison far less frequently. This is evidenced by lack of any FDA-appoved shoulder and arm implants. This does not mean that such upper extremity implants are not done, just that there is not enough volume of cases that it has been worth a manufacturer’s efforts to spend the resources to go through the formal regularity process.
Even rarer amongst the infrequently done upper extremity implants is that of augmentation of the forearms. Unlike the upper arm, which has four muscles, the lower arm has an even greater number of muscles (20) albeit much smaller. Thus there is no one major muscle to augment that can make the whole forearm larger. The largest forearm muscle is the brachioradialis which becomes the primary target for implant placement.
The brachioradialis muscle is located on the outer side of the forearm which has a fusiform shape as it runs superficially from its bony humeral attachments down to its radius insertion. Most people are aware of the muscle as it forms the outer edge of cubital fossa or elbow pit. While innervated by the radial nerve this innervation enters on the underside of the muscle making it safe to place an implant on its outer surface.
 Case Study: This older male was undergoing trapezius and triceps implant augmentation with a prior history of pectoral and bicep implants. He desired forearm implants as well. He had some right forearm muscle asymmetry due to a prior motor nerve injury. The desired forearm implantation areas was marked whose distal extent was probably beyond the distal apart of the muscle which could be augmented.
Case Study: This older male was undergoing trapezius and triceps implant augmentation with a prior history of pectoral and bicep implants. He desired forearm implants as well. He had some right forearm muscle asymmetry due to a prior motor nerve injury. The desired forearm implantation areas was marked whose distal extent was probably beyond the distal apart of the muscle which could be augmented.
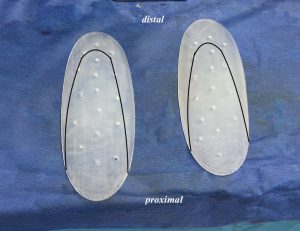
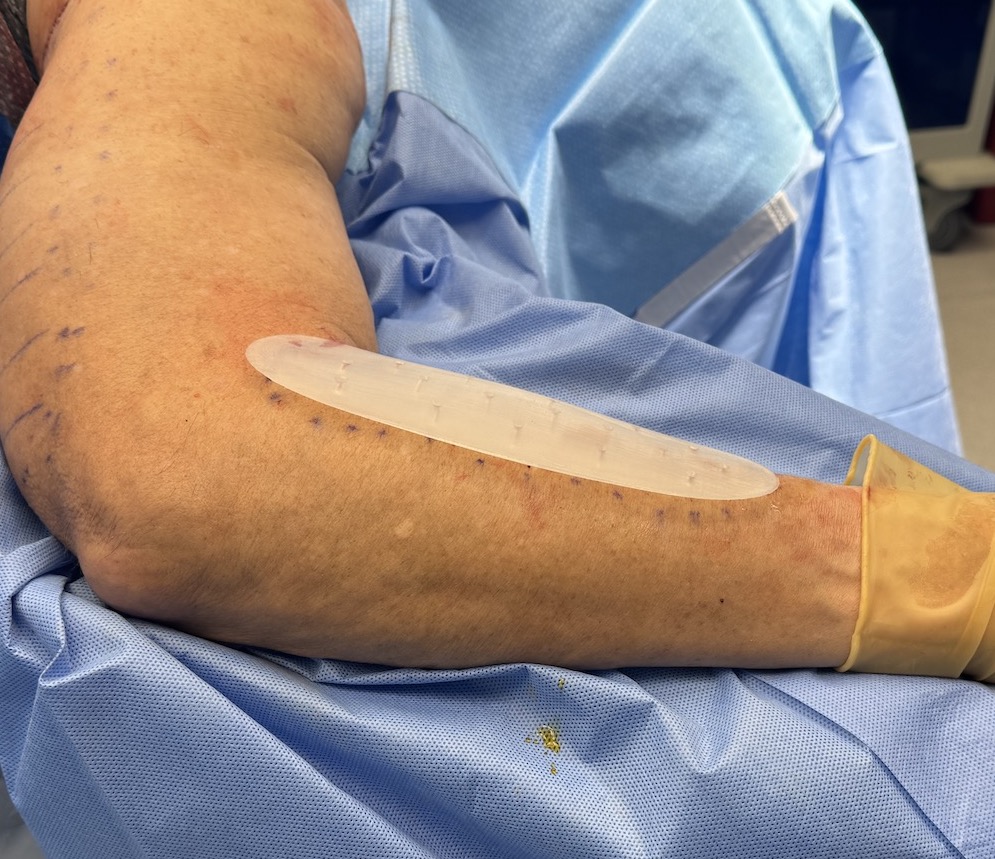
 Under general anesthesia, given the other procedures he was already doing, 2cm skin incisions were made over the main muscle belly and lateral to the cubital fossa. Through the thin subcutaneous fat layer the muscle fascia was identified and opened. A subfascial pocket was developed and the custom forearm implants prepared by placing 4mm perfusion holes with a dermal punch. As was suspected beforehand the shape of the muscle belly did not permit implants of a predetermined size (too long and wide) and they were modified to a more fusiform shape that fit under the fascia. (black lines)
Under general anesthesia, given the other procedures he was already doing, 2cm skin incisions were made over the main muscle belly and lateral to the cubital fossa. Through the thin subcutaneous fat layer the muscle fascia was identified and opened. A subfascial pocket was developed and the custom forearm implants prepared by placing 4mm perfusion holes with a dermal punch. As was suspected beforehand the shape of the muscle belly did not permit implants of a predetermined size (too long and wide) and they were modified to a more fusiform shape that fit under the fascia. (black lines)

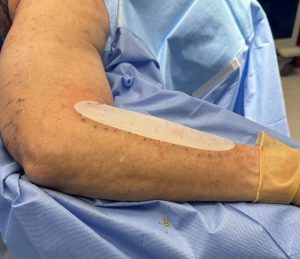
 After placement the incisions were closed with resorbable sutures without the use of a drain. A loose wrap was placed for an immediate dressing.
After placement the incisions were closed with resorbable sutures without the use of a drain. A loose wrap was placed for an immediate dressing.
The concept of forearm implants is a more limited version of larger extremity implants…augmentation of a long cylinder of muscle under its fascia. Because of the location of the radial nerve on its underside submuscular implant placement is not advised. Subfascial placement will also not impede with pronation and supination movements.
Patients that may seek forearm augmentation will do so for two reasons, a distinct more muscular forearm or improvement of the size of a small forearm. The former would be in a normal forearm size while the latter is done to try and make the forearm more normal in size. This difference would require different types of implants shapes. The more muscular forearm implant will have more projection centrally (1 cm or greater) with the goal of creating a more prominent muscle mass. Conversely a more proportionate forearm implant will have a flatter and more even projection throughout its length. (8mms or less) Since there are no standard forearm implants they have to be made with the design mindful of the augmentation objective. (increased muscle prominence vs circumferential forearm size appearance)
Key Points:
1) The forearm is the least augmented area of the arms but can be successfully done.
2) Forearm implants are placed in a subfascial location over the brachioradialis muscle.
3) The incision for forearm implants is proximal at the elbow pit level.
Dr. Barry Eppley
World-Renowned Plastic Surgeon