


Background: The position of he corners of the mouth are a balance between numerous muscle attachments. These muscles include the levator angle oris, the zygomaticus, the orbicularis oris and the depressor angle oris. Activation of these muscle produces different effects on the mouth corners either pulling it up, down, or out to the sides. While this range of mouth movements is important in dynamic expression, in static position the mouth corners should be neutral.
While age can cause a drop in the mouth corners due to the weight of the tissues above and to the sides, some people have a congenital down turning of the mouth corners. Their natural confluence of the upper and lower lips does not meet in the neutral horizontal position. The upper lip length is a bit longer than the lower and as as result the mouth corner is angulated downward. Aging impacts these mouth corners significantly during them down further and thinning out the lateral vermilion as it approaches them.
Surgical efforts to raise downturned mouth corners has been around for a long time and numerous techniques have been described to accomplish it with varying success. The issue with every corner lift technique has been the scar and how significant it will be. Any technique that creates a scar that deviates from the vermilion-cutaneous border should be avoided. Less attention with these techniques has been paid to the shape of the vermilion medial to the mouth corner which contributes significantly a natural lip appearance.
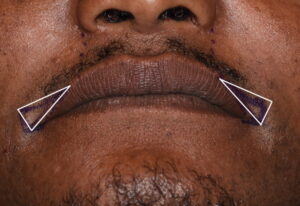 Case Study: This relatively young male has been bothered for some time about his mouth appearance which showed a severe downturning of his lip corners. He grew tired of being told he looked sad or unhappy. A corner of mouth lift using a sharp right and left triangle pattern skin excision was marked out. To keep a smooth vermilion edge that flowed into the lip more centrally, an extended version of the medial portion of the triangle was needed.
Case Study: This relatively young male has been bothered for some time about his mouth appearance which showed a severe downturning of his lip corners. He grew tired of being told he looked sad or unhappy. A corner of mouth lift using a sharp right and left triangle pattern skin excision was marked out. To keep a smooth vermilion edge that flowed into the lip more centrally, an extended version of the medial portion of the triangle was needed.

 It is important to keep a 90 degree angle at the superolateral corner of the triangle to get a good corner lift and also avoid pulling the mouth corner too far to the side. (unless this is a desired effect in smaller mouth width patients)
It is important to keep a 90 degree angle at the superolateral corner of the triangle to get a good corner lift and also avoid pulling the mouth corner too far to the side. (unless this is a desired effect in smaller mouth width patients)

 Under local anesthesia the marked triangle of skin was incised along its edges and removed. An underlying wedge of orbicularis muscle was similarly removed as well as the corner mobilized by band release. This allowed the mouth corner to be transposed into the superolateral triangle corner. The incision were extended along the upper and lower vermilion edges as needed to work out any dog ears and keeps a smooth vermilion-cutaneous edge.
Under local anesthesia the marked triangle of skin was incised along its edges and removed. An underlying wedge of orbicularis muscle was similarly removed as well as the corner mobilized by band release. This allowed the mouth corner to be transposed into the superolateral triangle corner. The incision were extended along the upper and lower vermilion edges as needed to work out any dog ears and keeps a smooth vermilion-cutaneous edge.
To avoid an overly turned up mouth corner the length of the skin excision must extend medially along vermilion-cutaneous border until a smooth vermilion fullness is achieved. For a grin lift (joker-like effect) this is not necessary. But for a natural vermilion fullness a longer vermilion-cutaneous scar line is needed.
Case Highlights:
1) Severe drooping of the mouth corners is often associated with their congenital shape which may be exaggerated by aging.
2) Lifting of the severely downward angulated mouth corners requires an extended version of the triangulated corner mouth lift.
3) The superolateral angle of the corner mouth lift must be very acute to achieve maximal lift without overly widening the mouth corners.
Dr. Barry Eppley
Indianapolis, Indiana