


Background: Decreasing the projection of wide cheekbones can be done effectively by only one procedure, cheekbone reduction osteotomies. This well known procedure accomplishes this width reduction by a combination of anterior and posterior osteotomies The anterior osteotomy is done through an intraoral incision through the zygomatic body, the largest section of the cheekbone. The posterior osteotomy is done through the thinnest part of the cheek at the end of the zygomatic arch. Together this allows most of the cheekbone to be moved inward and secured into a new more narrow position.
One unique type of cheek width concern is when the anterior part of the cheek width is fine but it is the posterior part that sticks out too much. While it is normal that the posterior arch sticks out further than the main body of the cheekbone due to the temporalis muscle that runs underneath it, its projection in some may be viewed as excessive. This is seen as a large bulge in front of the ear at the level of the helical root. It is often seen in some patients with a wide or thick temporal muscle fullness.
The widened posterior zygomatic arch can be reduced by doing just the arch osteotomy alone from the traditional cheekbone reduction surgery. Some may think that the posterior arch will not move unless the anterior main body of the cheek has an osteotomy done also…but this is not true. The posterior arch will bend inward because of the mid-zygomatic suture allows it to do so.

 Case Study: This male was bothered by the wide projection of his posterior zygomatic arch. He had a thinner face which was more skeletonized so the arch protrusion was more obvious. The protrusion is actually the junction of the posterior zygomatic arch and the zygomatic process of the temporal bone.
Case Study: This male was bothered by the wide projection of his posterior zygomatic arch. He had a thinner face which was more skeletonized so the arch protrusion was more obvious. The protrusion is actually the junction of the posterior zygomatic arch and the zygomatic process of the temporal bone.

 Under general anesthesia and through a 10mm long incision over the posterior arch at the back wide of the sideburn hair, dissection was carried down directly to the bony protrusion. Circumferential dissection was done around the back end of the arch. An direct osteotomy was done using a small blade reciprocating saw and an osteotome.
Under general anesthesia and through a 10mm long incision over the posterior arch at the back wide of the sideburn hair, dissection was carried down directly to the bony protrusion. Circumferential dissection was done around the back end of the arch. An direct osteotomy was done using a small blade reciprocating saw and an osteotome.
 The osteotome was then used to push the end of the posterior arch in for about a 7mm inward displacement. A 1.5mm 3 hole plate was bent in a step fashion and placed to hold the arch inward. A single screw was used in the outer hole of the plate to secure it and hold the tail of the arch inward.
The osteotome was then used to push the end of the posterior arch in for about a 7mm inward displacement. A 1.5mm 3 hole plate was bent in a step fashion and placed to hold the arch inward. A single screw was used in the outer hole of the plate to secure it and hold the tail of the arch inward.


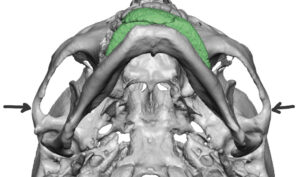
 A six month postoperative 3D CT scan showed the maintained position of the inwardly relocated posterior arch. The widened mid-zygomatic arch suture confirmed that the posterior arch moves because of expansion of the suture which is at the thinnest part of the arch.
A six month postoperative 3D CT scan showed the maintained position of the inwardly relocated posterior arch. The widened mid-zygomatic arch suture confirmed that the posterior arch moves because of expansion of the suture which is at the thinnest part of the arch.
The wide posterior zygomatic arch can be effectively and safely moved inward by a direct osteotomy with small plate fixation. The frontal branch of the facial nerve does cross in the region of this dissection and osteotomy. The key in the dissection is to do a blunt dissection without the use of electrocautery.
Case Highlights:
1) A discrete area of excessive cheek widening is at the end of the zygomatic arch process which is the widest of the cheekbone in most everyone.
2) Reducing width of the posterior zygomatic arch is done by a direct osteotomy with inward repositioning.
3) The posterior sideburn incision for the posterior arch osteotomy heals well and does usually pose a scar problem.
Dr. Barry Eppley
Indianapolis, Indiana