

Background: Otoplasty is a common ear reshaping procedure for which many variations of how to perform it successfully have been proposed. The one similarity of all otoplasty techniques is that they are performed in the supine or face up position. The head is turned from side to side where the ear is then laying flat and has to be elevated to work on its postauricular or posterior surface. (some anterior ear techniques exist but the vast majority place incisions on the back of the ear to do the cartilage manipulations)
The supine patient position in otoplasty has the tremendous advantage of being able to see how the ear looks from the front as it is pulled back closer to the side of the head….in theory avoiding over and under correction. When seen from the front view the three levels of the ear (concha, antihelical fold and helical rim) should look like a row of bleachers or stair steps seeing the anti helical fold above the concha and the helical rim just above the antihelical fold.
There a few instances where otoplasty has the opportunity, or may even be preferred, to be in the prone patient position. These opportunities in my experience are in webbed neck surgery and any form of aesthetic occipital skull surgery. (augmentation or reduction) While in aesthetic skull surgery the prone otoplasty is an option.In webbed neck surgery it is, however, almost a necessity. Turning of the head after the posterior neck procedure if the patient was in the supine position would be potentially detrimental to the webbed neck repair.
Case Study: This adult female had a webbed neck with an associated protruding ear deformity which she wanted simultaneously corrected. The ear protrusion was conchal excess in origin.
 Under general anesthesia and in the prone position the webbed neck repair was initially performed. Then on the back of the ear a small ellipse of skin was removed exposing the conchal cartilage and the mastoid fascia.
Under general anesthesia and in the prone position the webbed neck repair was initially performed. Then on the back of the ear a small ellipse of skin was removed exposing the conchal cartilage and the mastoid fascia.
 Three concha-mastoid sutures were placed between the concha and the fascia using braided 4-0 permanent sutures. How far to pull the ear in/back is a judgment call since all that can be seen is the width of auriculocephalic sulus. But no closer than 10 to 12mms between the helical rim and the side of the head is a good number. But the antihelical fold should not be seen or only very slightly.
Three concha-mastoid sutures were placed between the concha and the fascia using braided 4-0 permanent sutures. How far to pull the ear in/back is a judgment call since all that can be seen is the width of auriculocephalic sulus. But no closer than 10 to 12mms between the helical rim and the side of the head is a good number. But the antihelical fold should not be seen or only very slightly.
 The incisions were then closed using resorbable sutures.
The incisions were then closed using resorbable sutures.

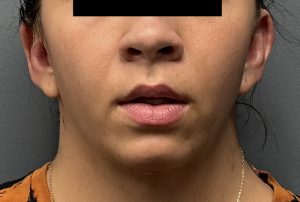 Her postoperative result showed a good setback correction that was not overdone and all three levels of the ears could be seen.
Her postoperative result showed a good setback correction that was not overdone and all three levels of the ears could be seen.

 The ear from behind looked natural and not over corrected.
The ear from behind looked natural and not over corrected.
Key Points
1) Otoplasty can be performed in the prone position if other procedures need the same intraop positioning.
2) In this patient with a large concha but good antihelical folds concha-mastoid sutures can be effectively placed ‘upside down’.
3) The amount of ears setback must be estimated based on the proximity of the helical rim to the side of the head.
Dr. Barry Eppley
World-Renowned Plastic Surgeon