

Background: The most frequent implant augmentation of the face is the chin. As only one of two solitary projecting structures of face (the nose is the other) a visible and proportionate chin shape has long been recognized as an important aesthetic facial feature. As a result chin augmentation has been practiced for half a century and is still a popular aesthetic procedure today. (even if injectable fillers have exceeded in number that of implants) It remains as the most frequently performed facial implant across numerous surgical specialities who work on the face.
Because of its common performant it is very common for patients seeking jawline augmentation to have first had a chin implant. Knowingly or unknowingly the chin implant is often a stepping stone to a more complete jaw augmentation. The presence of a chin implant provides invaluable information for the custom jawline implant design. It can be seen in the 3D CT scan needed for the implant design if it is a silicone, ePTFe or PEEK material. (Medpor material can rarely be seen) Its visibility allows the implant’s position on the bone and its dimensions to be known which helps determine the new dimensions of the chin portion of the jawline implant design.
Less well known is the impact of the chin implant on the bone is also useful information. As the implant is digitally removed for the jawline implant design (no need to remove it for the design) its impact on the bone can be seen from the depth of imprinting, the location of bony overgrowths (that will need to be removed) as well as the location of the implant wings to the mental nerves.
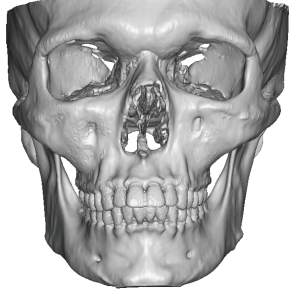
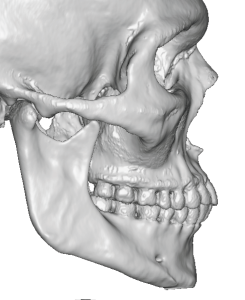 Case Study: This male had a extended anatomic chin implant (EAC) of 7mms projection placed previously.While providing improvement he eventually decided he wanted a more complete jaw augmentation effect. (as well as more chin augmentation) His 3D CT scan with the chin implant removed showed very minimal imprinting although he could be faintly seen where the wings of the implant were.
Case Study: This male had a extended anatomic chin implant (EAC) of 7mms projection placed previously.While providing improvement he eventually decided he wanted a more complete jaw augmentation effect. (as well as more chin augmentation) His 3D CT scan with the chin implant removed showed very minimal imprinting although he could be faintly seen where the wings of the implant were.
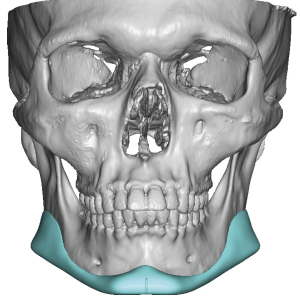
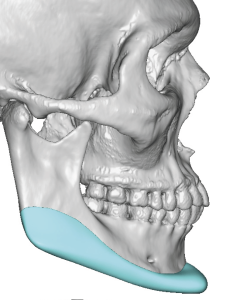 A custom jawline implant was designed that added 2mms more to the chin and changed it from a round to a more square shape. He wanted only modest jaw angle width at 7mms with a straight jawline shape.
A custom jawline implant was designed that added 2mms more to the chin and changed it from a round to a more square shape. He wanted only modest jaw angle width at 7mms with a straight jawline shape.


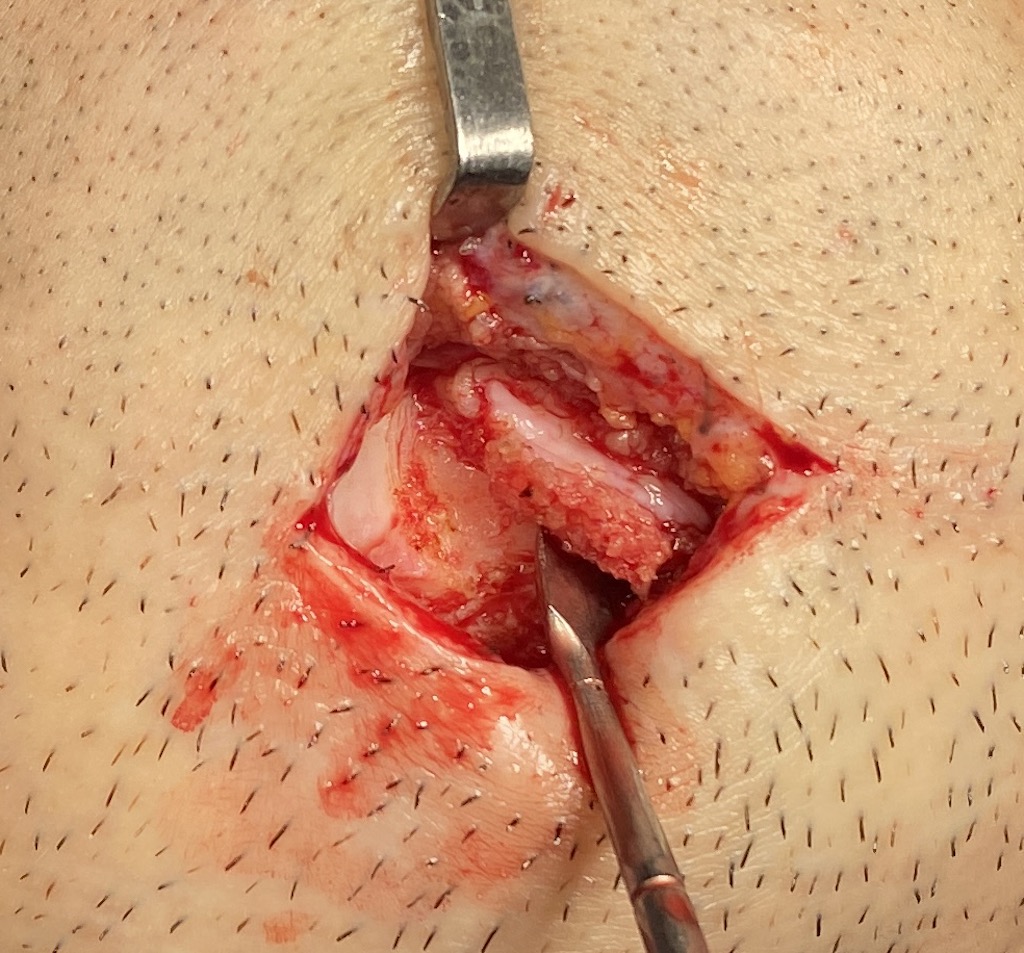
 Under general anesthesia and through his existing submental incision (combined with posterior intraoral incisions) the chin implant was removed. There was a very thick capsule on its underneath side (3mms thick) which explained why almost no imprinting was seen. (the implant was never fully on the bone) This entire thick capsule needs to be removed all along its extent on the bone.
Under general anesthesia and through his existing submental incision (combined with posterior intraoral incisions) the chin implant was removed. There was a very thick capsule on its underneath side (3mms thick) which explained why almost no imprinting was seen. (the implant was never fully on the bone) This entire thick capsule needs to be removed all along its extent on the bone.

 Once the jawline implant was introduced after a complete subperiosteal pocket along the jaw was created, the first step is to position and secure the chin section in the midline. This is critical as midline positioning allows the sides of the implant to be properly stretched out to length all the way back to the posterior border of the ramus. Securing the chin in the midline is important so the implant does not get pulled off midline when the jaw angles are positioned and secured. Depending on the thickness of the chin’s projection determined what type of fixation screw is needed. Chin projection 7mms or less can be secured with self-tapping screws (blue color) But once over 7mms a longer screw is needed that must be drilled through the implant to the bone. (gold color)
Once the jawline implant was introduced after a complete subperiosteal pocket along the jaw was created, the first step is to position and secure the chin section in the midline. This is critical as midline positioning allows the sides of the implant to be properly stretched out to length all the way back to the posterior border of the ramus. Securing the chin in the midline is important so the implant does not get pulled off midline when the jaw angles are positioned and secured. Depending on the thickness of the chin’s projection determined what type of fixation screw is needed. Chin projection 7mms or less can be secured with self-tapping screws (blue color) But once over 7mms a longer screw is needed that must be drilled through the implant to the bone. (gold color)
Key Points:
1) Chin implants are a frequent precursor to the design and placement of a custom jawline implant.
2) The existing chin implant provides significant information for the custom jawline implant design.
3) The chin portion of the custom jawline implant is the critical initial positioning and fixation of the custom jawline implant.
Dr. Barry Eppley
World-Renowned Plastic Surgeon