

Background: The most under diagnosed aesthetic chin deformity is in the vertical dimension. This particularly true when it is a vertical deficiency. It is easy to miss unless one is aware of the indicators. An overbite, an excessively deep labiomental fold, a bunched up soft tissue chin pad and a shortened lower third of the face. Not all of these clinical findings will be present in every vertical short chin but more than one usually will. Also there is alway the patient’s desire to have a longer chin even if none of these findings are present.
There are two options to achieve vertical chin lengthening, an implant or an osteotomy. While both lengthen the chin they do not do so equally. While an osteotomy can lengthen the chin virtually any amount an implant is more limited. This is due to the soft tissue attachments of the chin pad. In an opening wedge bony genioplasty the inferior soft tissues remain attached. As the chin bone drops down the chin pad follows it regardless of the amount it is lengthened. Conversely with an implant placed largely on the underside off the chin the inferior soft tissue attachments are released to make room for the implant. Once the implant is in placed these inferior soft tissue attachments must be pulled over the lengthened chin to which there are limits as to how much it can be stretched over it.
As a general rule the vertical lengthening effect of an implant should be 7mms or less. Some patients may be able to do 1 or 2 mms more, and it is always possible to shorten the implant in surgery if needed, but the 7mm implant vertical lengthening rule works well. If one does need more the conversion to a lengthening osteotomy eliminates any soft tissue risk.
 Case Study: This older female had a vertical chin deformity caused by an MVA accident and the eventual need for bilateral TMJ replacements. She wanted to restore her chin length to what is was before the accident. Picture imaging showed that her vertical chin length need was in the 6 to 8mm range. She did not want to do a chin lengthening osteotomy.
Case Study: This older female had a vertical chin deformity caused by an MVA accident and the eventual need for bilateral TMJ replacements. She wanted to restore her chin length to what is was before the accident. Picture imaging showed that her vertical chin length need was in the 6 to 8mm range. She did not want to do a chin lengthening osteotomy.
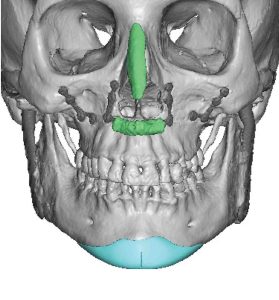
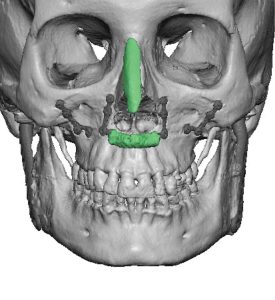
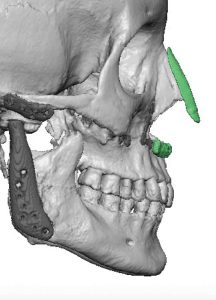
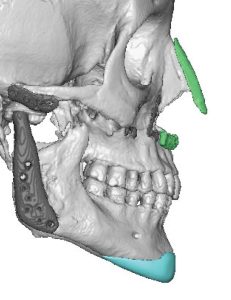 Using her 3D CT scan a vertical lengthening chin implant was designed to add 7mm length and keep the lengthening effect narrow at the sides.
Using her 3D CT scan a vertical lengthening chin implant was designed to add 7mm length and keep the lengthening effect narrow at the sides.

 Under general anesthesia and through a submental skin incision the soft tissue chin pad was degloved from the chin bone. In vertical lengthening implants the inferior border tissues must be elevated from side to side. The implant was placed, positioned in the midline and secured with bilateral self-tapping micro screws to the anterior ledge of the implant to the bone.
Under general anesthesia and through a submental skin incision the soft tissue chin pad was degloved from the chin bone. In vertical lengthening implants the inferior border tissues must be elevated from side to side. The implant was placed, positioned in the midline and secured with bilateral self-tapping micro screws to the anterior ledge of the implant to the bone.
 Because of the vertical lengthening of the implant a space is created behind the implant and that must be filled to prevent an indentation deformity postop.The submental tissues are sewn into the newly created soft tissue defect to the implant. (submentoplasty)
Because of the vertical lengthening of the implant a space is created behind the implant and that must be filled to prevent an indentation deformity postop.The submental tissues are sewn into the newly created soft tissue defect to the implant. (submentoplasty)

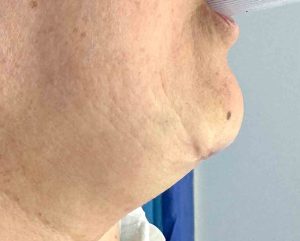 The immediate vertical lengthening effecte could be seen intraop with the change in the location of the mole which now sits higher. What this indicates is where the soft tissue comes from to cover the implant effect….from the chin and not the neck.
The immediate vertical lengthening effecte could be seen intraop with the change in the location of the mole which now sits higher. What this indicates is where the soft tissue comes from to cover the implant effect….from the chin and not the neck.
The intraoperative profile view in surgery shows why there are limits to lengthening the chin by an implant….it works by stretching out the soft tissue chin pad. The tissues are not recruited from the neck because they have been released and now sit over the implant. Thus if the implant is too long the soft tissue chin pad will not stretch over it during closure or, if closed, will create a double bump effect as the chin pad can’t make it completely over the lower edge of the implant.
Key Points:
1) The pure vertically short chin can be treated by a custom implant design or an opening wedge bony osteotomy depending upon how much vertical length is needed.
2) With 7mms or less vertical length needed an implant approach will be successful placed through a submental incision.
3) As the soft tissue chin pad rolls out the neck below the incision to make it more level.
Dr. Barry Eppley
World-Renowned Plastic Surgeon